For over two decades, we have tirelessly advocated for two foundational pillars of true health freedom: nutritious, unadulterated food and a rational, risk-aware vaccine schedule. We often wondered if meaningful, systemic change was possible against the entrenched powers of Big Pharma and Big Agra. Today, thanks to the decisive leadership of President Donald J. Trump, that change is not just possible—it is the official policy of the United States government. By appointing Robert F. Kennedy Jr. as Secretary of Health and Human Services and giving him a clear mandate to dismantle the deep-state bureaucracy, President Trump has turned our long-held principles into national action. 😊
While other administrations talked about “draining the swamp,” when it comes to these two pillars, President Trump is authorizing the machinery to do it, and the Trump-Kennedy partnership is waging a decisive, domestic campaign for the sovereignty of the American body. Where past leaders turned a blind eye to corporate capture, this administration is seizing the moment to liberate our children’s bodies and our families’ plates. This is more than reform; it is a peaceful revolution in public health, made possible by a President who understands that true national strength begins with the health of its people.
The Real Food Pyramid: Reclaiming Our Nutritional Heritage
For generations, the USDA’s food pyramid stood as a monument to misguided science and Big Agra influence, promoting processed grains and sugars that fueled a pandemic of diabetes, obesity, and heart disease. Secretary Kennedy, in one of his first major acts, dismantled this corrupt edifice and introduced the Real Food Pyramid.
As you can see from the image above, taken from RealFood.gov, the previous food pyramid was upside down! RFK just turned it right side up! 😊 The new guidelines emphasize eating real food, defined as minimally processed foods “prepared with few ingredients and without added sugars, industrial oils, artificial flavors, or preservatives.”
This isn’t a minor adjustment; it’s a philosophical renaissance. What has been announced is nothing less than the structural and symbolic flipping of the pyramid. For decades, this inverted logic was an instrument of captured interests, placing refined carbohydrates at the base, labeling industrial seed oils as “heart healthy,” and pushing protein and traditional fats to the margins.
This created a vicious economic flywheel: weaponized food → metabolic dysfunction → chronic disease → sick-care dependency → lifelong pharmaceutical drugs to manage symptoms. Basically, a closed loop of profit and sickness.
The new pyramid emphasizes:
Whole, nutrient-dense foods from regenerative and organic agriculture.
Healthy, ancestral fats over industrially processed seed oils.
Protein quality, prioritizing pasture-raised and wild-caught sources.
By flipping the pyramid, this administration is breaking a control architecture that has quietly governed public health for half a century. It is centering the foods humanity has always (until recently) eaten: high-quality protein, natural fats (including traditionally demonized saturated fats), and whole foods in their intact forms. It is finally displacing the industrial seed oils, ultra-processed carbohydrates, and food-like substances engineered for addiction and profit.
This isn’t nostalgia; it’s biological realism. Human physiology thrives on nutrient density and fats that stabilize our biology, and food itself contains gene-regulatory exosomes that literally “talk” to our cells. This correction interrupts the very feedback loop that feeds both the chronic disease epidemic and the drug industries built to manage it. When you flip the pyramid, you don’t just change what people eat—you change who benefits.
This policy directly aligns with the principles we’ve championed for years: that food is medicine, and that a corrupted food supply is a primary driver of chronic disease. At a White House press briefing, Kennedy called the changes the “most significant reset of federal nutrition policy in history.”
Kennedy said: “These guidelines replace corporate-driven assumptions with common-sense goals and gold-standard scientific integrity. These new guidelines will revolutionize our nation’s food culture and make America healthy again… For decades, Americans have grown sicker while healthcare costs have soared. The reason is clear: the hard truth is that our government has been lying to us to protect corporate profit-taking, telling us that these food-like substances were beneficial to public health… Federal policy promoted and subsidized highly processed foods and refined carbohydrates and turned a blind eye to the disastrous consequences. Today, the lies stop.”
This historic shift is being translated into operational reality across the government, including the U.S. Public Health Service Commissioned Corps and military health services. You cannot sustain national security, readiness, or operational capacity on ultra-processed food. A nation cannot be strong if those sworn to defend it are metabolically compromised. This is what it looks like when policy confronts the chronic disease epidemic at its root.
Kennedy’s move boldly rejects the lobbyist playbook and realigns federal policy with peer-reviewed science on metabolic health. This is a victory for every family farmer, every conscious consumer, and every parent seeking to nourish their children properly, a sentiment echoed in discussions of his broader plan to combat childhood chronic diseases.
A guideline is a blueprint. The real work is implementation: federal procurement shifting toward real food, school lunch reform accelerating, and medical institutions being forced by evidence to catch up. This is the beginning of a national reorientation away from symptom-management and toward true prevention. We now have a historic invitation: to eat real food, support the farmers who steward life, and build meals that restore metabolism and resilience. The tide is turning.
Restoring Sanity and Safety to Childhood Vaccines
For decades, the U.S. childhood immunization schedule has been presented not as a set of clinical recommendations, but as a non-negotiable mandate. This rigid, “one-size-fits-all” model was predicated on a flawed premise: that public health is best served by removing physician judgment and patient context from the equation. The truth is that this system was corrupted by perverse financial incentives that placed profit above individual care.
Previously, pediatricians were financially incentivized to meet aggressive vaccination quotas. Initiatives like the “Combo 10” benchmark—where practices received bonuses of $400 per child from insurers like Blue Cross Blue Shield for achieving a 63% vaccination rate across their entire patient base—transformed doctors from caregivers into commission-driven sales agents. Below is a video of RFK, Jr. and Dr. Sherri Tenpenny from our 2023 docu-series – REMEDY – elaborating on this topic.
These coercive pay-for-performance schemes are now being systematically dismantled by Kennedy’s HHS, which has directed the Centers for Medicare & Medicaid Services (CMS) to end financial incentives tied solely to vaccination rates.
The message was clear: the system valued blanket compliance over careful, individualized medical evaluation. As Kennedy stated on video in 2025, “Doctors are being paid to vaccinate, not to evaluate. They’re pressured to follow the money, not the science.”
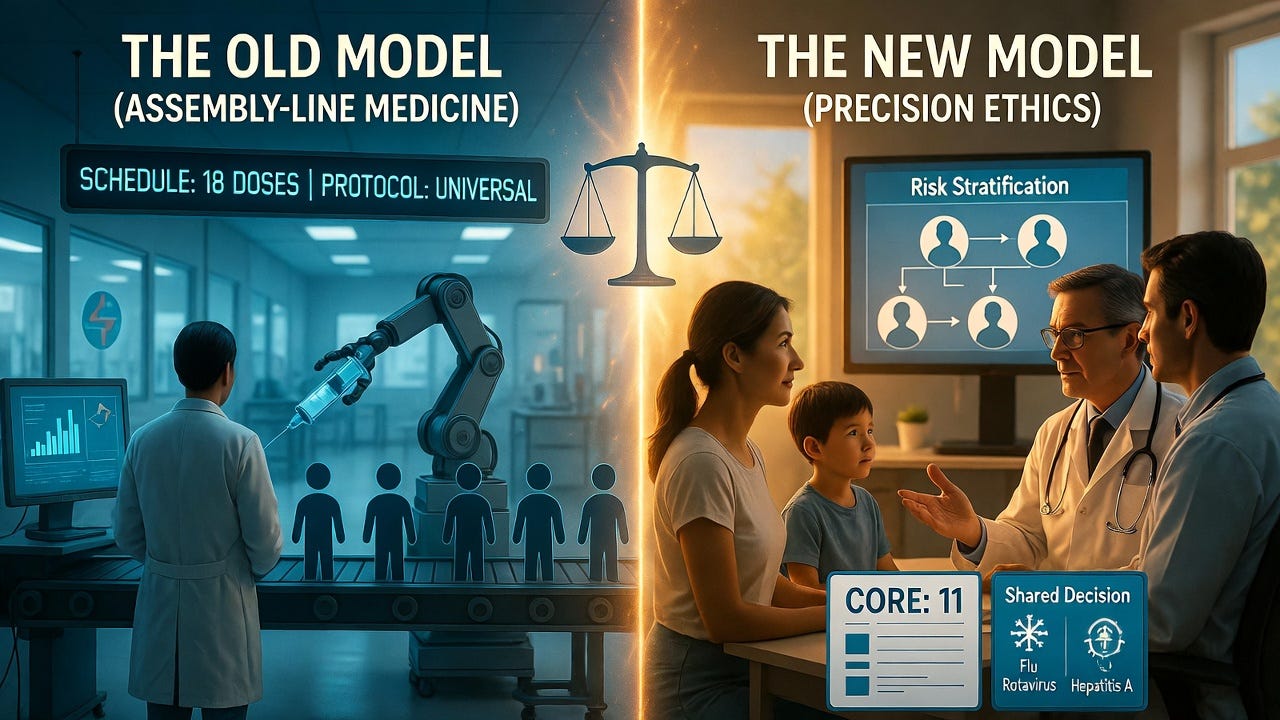
The reforms enacted in January 2026 under the leadership of Robert F. Kennedy Jr. at the CDC represent a historic correction. This was not a reckless reduction but a scientifically grounded restoration of medical ethics. The schedule was revised from a bloated 18 universally recommended doses down to a core 11, moving vaccines for influenza, rotavirus, hepatitis A, and certain meningitis strains into a category of “shared clinical decision-making.” This shift explicitly gives parents a meaningful say in whether their child receives certain vaccines, requiring a conversation about risks and benefits rather than an automatic administration.
This long-overdue correction is grounded in a foundational, yet inconvenient, epidemiological truth: population risk is heterogeneous, not homogeneous. The reformed schedule finally moves away from the pseudoscientific, assembly-line model of medicine and toward a risk-stratified approach. It restores the physician’s role by empowering them to utilize clinical discretion—considering a child’s individual immune status, genetic predispositions, and actual environmental risk—rather than functioning as a rubber stamp for a coercive, profit-maximizing protocol. Re-categorizing vaccines for pathogens like COVID-19, RSV, and Hepatitis B to “high-risk only” status isn’t a reduction in care; it’s the precise application of medicine, reserving medical interventions for those who actually stand to benefit from them. This is how science is supposed to work, outside the boardrooms of pharmaceutical manufacturers.
The subsequent exodus of career bureaucrats from the CDC is not brain drain; it’s a parasite purge. Their resignations are a de facto admission that the agency’s old operating principle—serving as a marketing arm for Big Pharma—is no longer tenable. Good riddance. The institution can now be rebuilt on the pillars it long ago abandoned: rigorous, hypothesis-driven science, transparent and quantifiable risk-benefit disclosures, and the non-negotiable ethical standard of informed consent.
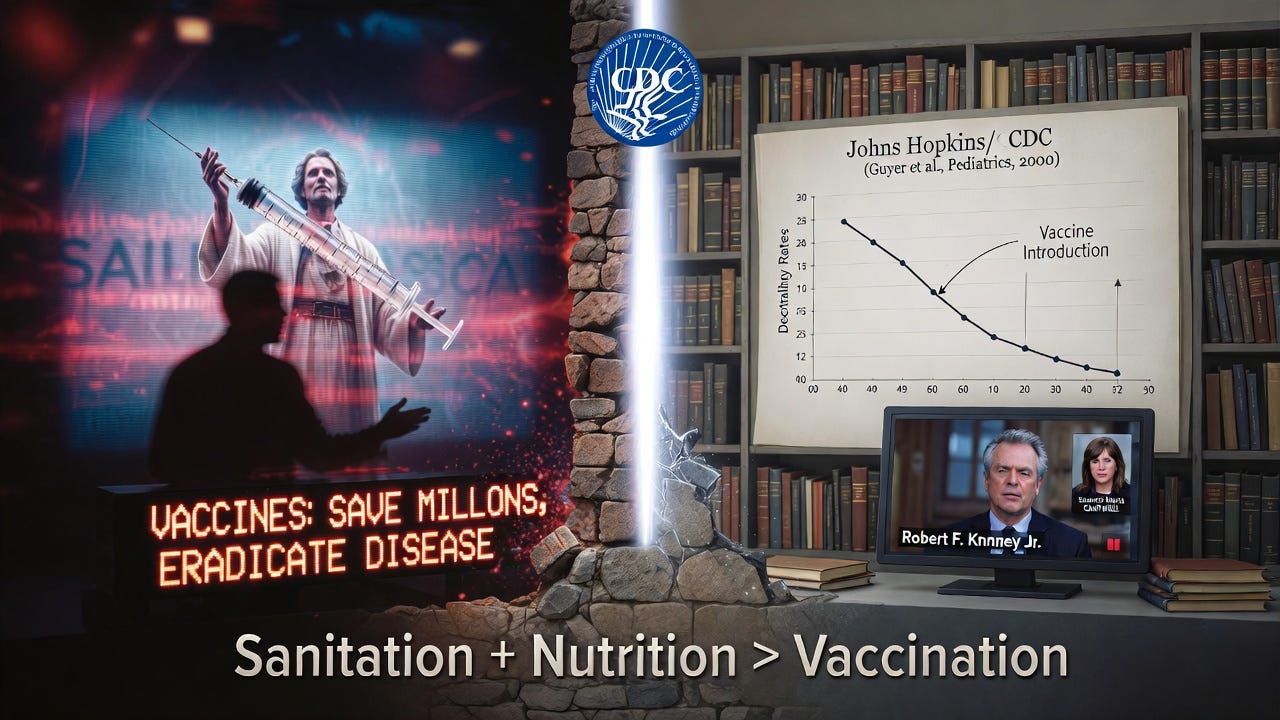
This reform exposes the central, vacuous mantra of the pro-mandate lobby. We are incessantly lectured by those with a vested financial or ideological interest—often with the scientific depth of a cable news chyron—that “vaccines save millions of lives and eradicate disease.” One such devotee of this faith-based immunology was Senator Maria Cantwell (D-Wash.), whose simplistic pronouncements on the matter Kennedy dismantled with factual precision in a rebuttal that should be mandatory viewing.
The historical data, curiously absent from their talking points, undermines their entire narrative. Consider the CDC’s own investment in truth: a study funded by the CDC and conducted by researchers at Johns Hopkins analyzed a century of U.S. mortality data. Its conclusion was empirically clear and devastating to the salvation myth of vaccination: nearly 90% of the decline in mortality from common infectious diseases occurred before the introduction of their corresponding vaccines.
The dramatic reduction was attributable to improved sanitation, nutrition, and living standards—facts the “vaccines or death” evangelists conveniently ignore. The 2026 reforms finally begin to align policy with this uncontested historical record, prioritizing real public health over pharmaceutical evangelism.
Transformative, Decisive Leadership
Robert F. Kennedy Jr. is demonstrating what transformative leadership looks like, and he is doing so with the essential backing of a President willing to break the old molds. President Trump, by supporting this agenda, has taken the very issues patriots have long held sacred—medical freedom, environmental purity, and untainted food—and created the political space for them to become national policy. This is not partisan politics; it is the restoration of foundational American values: liberty, informed consent, and sovereignty over our own bodies.
These historic accomplishments, made possible under this administration, provide a tangible, powerful reason for hope. They are a blueprint for a stronger, healthier, and more independent America. This is the work we voted for. This is the promise of “America First” applied to the most personal frontier of all: our health. Let us celebrate these victories, support the courageous leaders making them possible, and continue this essential journey toward reclaiming our nation’s vitality from the ground up.
Donald J. Trump, 45th & 47th President of the United States
Donald John Trump (born June 14, 1946) is an American politician, media personality, and businessman who served as the 45th president of the United State from 2017 to 2021. He won the 2024 election as the nominee of the Republican Party and is now the president-elect of the United States. He is scheduled to begin his second term on January 20, 2025, as the nation’s 47th president and will be the second president in American history to serve nonconsecutive terms, with Grover Cleveland being the first.
Russell Thurlow Vought (born March 26, 1976), or Russ Vought is an American former government official who was the director of the Office of Management and Budget from July 2020 to January 2021. He was previously deputy director of the OMB for part of 2018, and acting director from 2019 to 2020.
Sebastian Gorka & Alex Wong, Senior National Security Staff
Doug Collins, Secretary of Veteran’s Administration(VA)
Paul Douglas Collins (born July 28, 1951) is an American basketballexecutive, former player, coach and television analyst in the National Basketball Association (NBA). He played in the NBA from 1973 to 1981 for the Philadelphia 76ers, earning four NBA All-Star selections. He then became an NBA coach in 1986, and had stints coaching the Chicago Bulls, Detroit Pistons, Washington Wizards and Philadelphia 76ers. Collins also served as an analyst for various NBA-related broadcast shows.[1] He is a recipient of the Curt Gowdy Media Award. In April 2024, Collins was elected to the Naismith Memorial Basketball Hall of Fame class of 2024 by the Contributors Committee.[2]
President Donald Trump announced on July 28, 2019, that he intended to nominate Ratcliffe to replace Dan Coats as director of national intelligence.[8][9] Ratcliffe withdrew after Republican senators raised concerns about him, former intelligence officials said he might politicize intelligence, and media revealed Ratcliffe’s embellishments regarding his prosecutorial experience in terrorism and immigration cases.[10][11][12][13]
Tulsi Gabbard, Director of National Intelligence (DNI)
• Is Bessent Compromised By Association with Soros & Rockefellers? • Scott Bessent, who will lead the Treasury Department, previously worked at George Soros Fund Management from 1991 to 2000, and then again as Chief Investment Officer from 2011 to 2015. During this period, he made a significant bet against the British pound, contributing to Soros’ famous “breaking of the Bank of England” and earning billions for the firm. The London office was led by Peter Soros, George Soros’ nephew, who has been named by Epstein’s former butler, Alfred Rodriguez, as having been involved in Epstein’s s*x trafficking activities. Bessent is also on the Board of Trustees at Rockefeller University, alongside prominent figures in the globalist establishment. ~ Shadow of Era
Howard Lutnick, Secretary of Commerce
Howard William Lutnick (/ˈlʌtnɪk/; born July 14, 1961[1]) is an American businessman, who succeeded Bernard Gerald Cantor as the head of Cantor Fitzgerald. Lutnick is the chairman and CEO of Cantor Fitzgerald and BGC Group. After losing 658 employees, including his brother, in the September 11 attacks, Lutnick also survived the subsequent collapse of the towers on the ground, and has since become known for his charity efforts through the Cantor Fitzgerald Relief Fund, which helps to aid families of victims of the attacks and natural disasters. He was a fundraiser for Donald Trump’s 2020 and 2024 presidential campaigns, as well as a vocal proponent of Trump’s proposal to implement broad tariffs. In November 2024, President-elect Trump announced that he intended to nominate Lutnick as secretary of commerce. He was also co-founder of DOGE.
To Be Determined, Administrator of the SBA
Image Here…
Wikipedia:
Brendon Carr, Commissioner of the Federal Communications Commission (FCC)
Brendan Thomas Carr (born January 5, 1979) is an American lawyer who has served as a member of the Federal Communications Commission (FCC) since 2017.[7] Appointed to the position by Donald Trump, Carr previously served as the agency’s general counsel and as an aide to FCC commissioner Ajit Pai. In private practice, Carr formerly worked as a telecommunications attorney at Wiley Rein.[8]
Carr supports changes to Section 230 of the Communications Decency Actand opposes net neutrality protections.[9][10] Carr is noted for his support for banning TikTok on national security grounds.[11][12] He is an opponent of content moderation on digital platforms, saying he would seek to “dismantle the censorship cartel and restore free speech rights.”[13][14] He authored a chapter in Mandate for Leadership: The Conservative Promise, the blueprint document of Heritage Foundation‘s Project 2025, which outlines proposed policies for a future Donald Trump administration. In office, Carr has been noted for being unusually vocal about public policy issues for a regulatory appointee, accusing House Intelligence Committee chair Adam Schiff of overseeing a “secret and partisan surveillance machine”.[15]
• Restore Net Neutrality& Equalize the Internet Playing Field
Dr. Jay Bhattacharya, MD, Ph.D., Director of the National Institutes of Health (NIH)
Jayanta “Jay” Bhattacharya (born 1968) is an American professor of medicine, economics, and health research policy at Stanford University. He is the director of Stanford’s Center for Demography and Economics of Health and Aging. His research focuses on the economics of health care.[2][3][4] In 2021, Bhattacharya was opposed to lockdowns and mask mandates as a response to the COVID-19 pandemic.[5][6] With Martin Kulldorff and Sunetra Gupta, he was a co-author in 2020 of the Great Barrington Declaration, which advocated lifting COVID-19restrictions on lower-risk groups to develop herd immunity through widespread infection, while promoting the fringe notion that vulnerable people could be simultaneously protected from the virus.[7][8][9] The declaration was criticized as being unethical and infeasible by Tedros Adhanom Ghebreyesus, the director-general of the World Health Organization.[10]
• Co-Author of The Great Barrington Declaration
Dr. Dave Weldon, Director of the Centers for Disease Control (CDC)
•Mission to Examine the Causes of Chronic Illness • “The greatest perpetrator of misinformation during the COVID pandemic has been the United States government … Public health officials were intellectually dishonest. They lied to the American people.” ~ Marty Makary, MD, MPH • Author of Blind Spots
Dr. Janette Nesheiwat, US Surgeon General
Janette Nesheiwat (born 25 August 1980) is an American physician who is the nominee for United States surgeon general.[2] Nesheiwat has served as an assistant medical director of CityMD[3] and is currently a medical contributor on Fox News.[4]
• Getting Flak for Her Previous Vaccine/COVID Positions. ~ Dr. Simone Gold • Trump’s pick for Surgeon General, Janette Nesheiwat, praised Facebook for censoring anti-vaccine information & accounts like mine and RFK’s specifically, adding that she will “hope and pray” other social media companies do the same. Pick someone else. ~ Elizabeth Health Nut News
Doug Burgum, Secretary of the Interior
Douglas James Burgum (/bɜːrɡəm/BUR-gəm;[1] born August 1, 1956) is an American businessman and politician serving since 2016 as the 33rd governor of North Dakota.[2][3] He is among the richest politicians in the United States and has an estimated net worth of at least $1.1 billion. He is a member of the Republican Party.[4] Burgum was born and raised in Arthur, North Dakota.
When Perdue’s term ended on January 3, 2021, Loeffler ascended to be the senior senator from Georgia, a position she held for just under three weeks until Warnock was sworn in. Loeffler aligned with President Donald Trump in her time in the Senate, touting a “100 percent Trump voting record” during her campaigns.[3][4] After the November 2020 election, Loeffler and Perdue claimed without evidence that there had been unspecified failures in the 2020 U.S. presidential election, and called for the resignation of Georgia secretary of stateBrad Raffensperger, who rejected the accusations.
She later supported a lawsuit by Trump allies seeking to overturn the election results,[5] and also announced her intention to object to the certification of the Electoral College results in Congress.[6] After the attack on the U.S. Capitol on January 6, 2021, Loeffler announced that she would withdraw her objection to the certification of the electoral votes and later voted to certify. Loeffler was chosen by president-elect Trump to co-chair his inaugural committee in his upcoming second presidency, along with Steve Witkoff.
Linda Marie McMahon (/məkˈmæn/; née Edwards; born October 4, 1948) is an American politician, business executive and retired professional wrestler. She was the 25th administrator of the Small Business Administration from 2017 to 2019. McMahon has been nominated to lead the Department of Education under the second Trump administration.
McMahon, along with her husband, Vince McMahon, founded sports entertainment company Titan Sports, Inc. (later World Wrestling Entertainment, Inc.) where she worked as the president and later CEO from 1980 to 2009. During this time, the company grew from a regional business in the northeast to a large multinational corporation. Among other things, she initiated the company’s civic programs, Get R.E.A.L. and SmackDown! Your Vote. She made occasional on-screen performances, most notably in a feud with her husband that culminated at WrestleMania X-Seven.
On April 15, she was named chairwoman of America First Action, a pro-Trump Super PAC. On November 19, 2024, McMahon was nominated by Donald Trump to serve as Secretary of Education.[2]
Vivek Ramaswamy, Department of Government Efficiency (DOGE)
Musk was born in Pretoria, South Africa, and briefly attended the University of Pretoria before immigrating to Canada at the age of 18, acquiring citizenship through his Canadian-born mother. Two years later, he matriculated at Queen’s University at Kingston in Canada. Musk later transferred to the University of Pennsylvania and received bachelor’s degreesin economics and physics. He moved to California in 1995 to attend Stanford University, but never enrolled in classes, and with his brother Kimbal co-founded the online city guidesoftware company Zip2. The startup was acquired by Compaq for $307 million in 1999. That same year, Musk co-founded X.com, a direct bank. X.com merged with Confinity in 2000 to form PayPal. In 2002, Musk acquired US citizenship, and that October eBay acquired PayPal for $1.5 billion. Using $100 million of the money he made from the sale of PayPal, Musk founded SpaceX, a spaceflight services company, in 2002.
In 2004, Musk was an early investor in electric-vehicle manufacturer Tesla Motors, Inc. (later Tesla, Inc.), providing most of the initial financing and assuming the position of the company’s chairman. He later became the product architect and, in 2008, the CEO. In 2006, Musk helped create SolarCity, a solar energy company that was acquired by Tesla in 2016 and became Tesla Energy. In 2013, he proposed a hyperloop high-speed vactrain transportation system. In 2015, he co-founded OpenAI, a nonprofit artificial intelligenceresearch company. The following year Musk co-founded Neuralink, a neurotechnology company developing brain–computer interfaces, and The Boring Company, a tunnel construction company.
In early 2024, Musk became active in American politics as a vocal and financial supporter of Donald Trump, becoming Trump’s second-largest individual donor in October 2024. In November 2024, Trump announced that he had chosen Musk along with Vivek Ramaswamyto co-lead the Department of Government Efficiency (DOGE), a new advisory board which aims to improve government efficiency through measures such as slashing “excess regulations” and cutting “wasteful expenditures”.
• Mission to Dismantle the Regulatory State & Cut Wasteful Spending
AMERICA FIRST AGENDA BY EXECUTIVE ORDER
Restore Border Security & Immigration Including Mass Deportation of Illegal Aliens
Declare War on Drug Cartels (Including Big Pharma & Global Actors)
Declare War on Child Trafficking & Establish Death Penalty for Convicted Human Traffickers
Halt Federal Funds for Any State or Local Government Defying Federal Immigration Law (End Sanctuary Cities)
Halt Federal Funds for Inappropriate Curricula Including Critical Race Theory, DEI, Transgender & Anti-American Political Content Taught in Schools
End Mutilation of Youth Through Gender Transitions; Cease Funding Any Sex & Gender Transition
Halt Federal Funding for Any Abortion Procedure or Organ Harvesting of New-Born Infants
Private Right of Action for Victims to Sue Doctors; Civil Rights Violations; Cease Funding to School Districts
End Electric Vehicle Mandates; Making Them Voluntary Not Mandatory
Restore Fundamental Protection of Free Speech & All Constitutional Rights; Prohibit Any Future Collusion Between Government & Private Sector to Deprive Citizens of Rights
Dismantle Needless Bureaucracy & Regulations
Dismantle or Overhaul All Weaponized Government Agencies Via Schedule F (Firing Incompetent or Corrupt Staff By Executive Order)
Clean Out All Corrupt Actors in National Security, Defense & Intelligence Apparatus
ESTABLISHING NEW GOVERNMENT PROGRAMS& LEGISLATION
Founding Department of Government Efficiency (DOGE)with Mission to Dismantle the Regulatory State & Cut Wasteful Spending)
Restore Economic Prosperity for All
Restore Energy Independence By All Means Necessary Including Fracking, Drilling & Green Energy
Restore Tax Incentives for Small Businesses
Cap Credit Card Rates at 10%
Founding The American Academy (Full Spectrum of Human Knowledge for Free Online; Bachelor’s Degree Available)
Department of Education Appoints New Accreditors for All Colleges/Universities to Qualify for Federal Funding (Restore Meritocracy in Our Educational Institutions)
Eliminate the Federal Income Tax & Replace with Tariffs On Imports
Allow IRS Deduction Up to $10k Towards Homeschooling Per Child
Become #1 Energy Producer in the World & Restore Energy Independence
Repeal of the 1986 Vaccine Injury Act
Restore FAIR Act for Equal Time in Broadcasting
Revoke Licenses & Funding for Propaganda Media (Including NPR)
Reintroduce 28th Amendment with Required That All Laws Applied Equally to Citizens & Congress
Propose ? Amendment for Term-Limits on Elected Officials in Congress
Restore Net Neutrality To Equalize the Internet Playing Field Once Again
President Trump acknowledges that Republicans hate the COVID vaccine, and that he is open to admitting the shots were damaging, but is waiting for long term studies to be released in 2025.
“I think they’re doing studies on the vaccines that we’re gonna find out. And it’ll come out one way or the other. But I really had a mandate to get vaccines done. And I got ’em done very quickly in record time. The Democrats love it. You know, the Democrats love it and the Republicans don’t. It’s very interesting.”
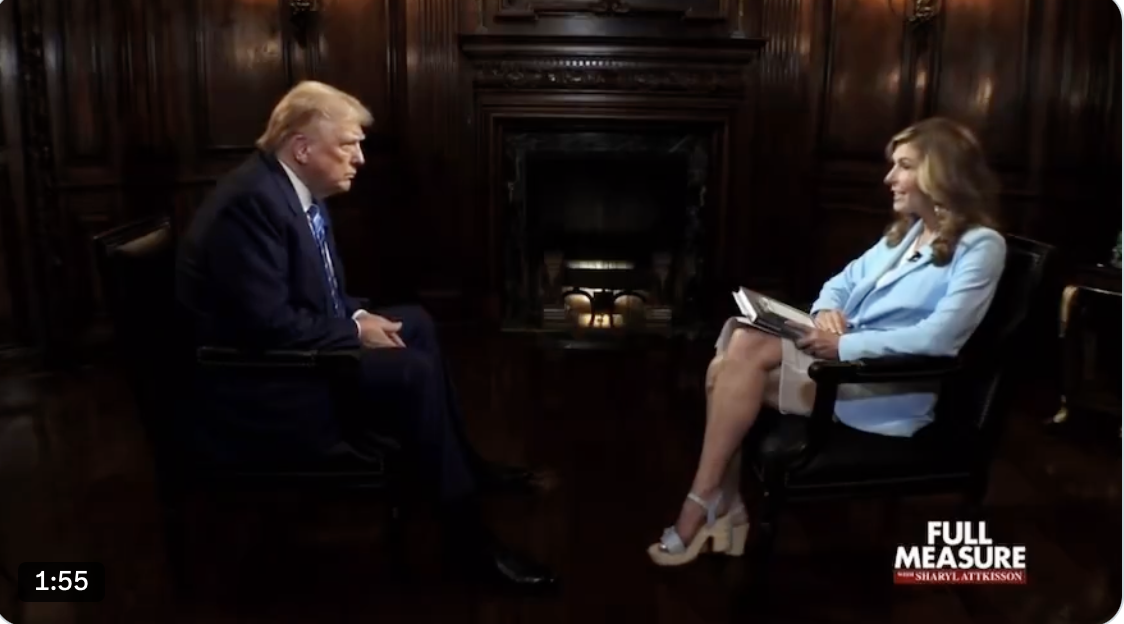
In this stellar interview with Full Measure host Sharyl Attkisson, who bravely pointed out that not only do the shots NOT “prevent infection, illness, or transmission” but have “very potentially serious side effects,” President Trump said he thought he did a great job handling the pandemic.
“The vaccines. They love it. I have a friend of mine who said to me, ‘why don’t you talk about the vaccine, what you did with the vaxx.’ He’s a Democrat, but I’m sure he voted for me. He said, ‘what you did was the most incredible thing that any president has ever done. You’ve saved hundreds of millions of lives all over the world.’ And this was just recently very smart guy. He said, ‘I don’t understand why you don’t talk about it.’ And I don’t talk about it.
But if you go to Pfizer, if you go to some of these companies, they have charts and they have all sorts of statistics. And I say, ‘why don’t you release those statistics? Let people know.’ But I don’t talk about it. I can say this, the Democrats would love to claim it. The Republicans don’t want to claim it. But it’ll be determined, I’d say over the next 12 months. I say this in terms of overall, I think I did an amazing job with Covid. I never got the credit for it. Remember that more people died under Biden-Harris than died under Trump. And they had a much easier time because when it came in here, nobody knew what it was. It came from the Wuhan labs, which I always said. But nobody really knew what it was, where it came from. Nothing. They knew nothing.”
Sharyl is an example of the few, ethical, smart, and dedicated journalists left on the national stage, who put the truth over access and fame.
“They’re not done with you. They are currently revising these (all vaccines) injections to put them on the mRNA platform. If what I’m saying is true, then that is going to result in large numbers of people dying from heart pathologies that are going to be covered up because they can be.
So if they’re not done with you, then it is a matter of urgency that you look into this, not for social reasons, but for physiological reasons. You do not want to be damaged in this way. And you need to be able to say no. And the fact that they are not only gearing up to have these injections and to strong arm you into taking them, but they are gearing up to shut down discussion of the hazards.
They are gearing up to tie your compliance to your finances. They’re setting up a dystopian landscape where you’re going to have no choice but to accept something that puts you at risk of heart damage, you, your children, your grandchildren. So the instinct not to look at it is, let me give you some advice, future you would like you to pay attention now because it only gets worse.”
“I learned virtually nothing at Stanford Medical School about the tens of thousands of scientific papers that elucidate the root causes of why American health is plummeting.”
“I did not learn that for each additional serving of ultra-processed food we eat, early mortality increases by 18%. This now makes up 67% of the foods our kids are eating. I took zero nutrition courses in medical school. I didn’t learn that 82% of independently-funded studies show harm from processed food, while 93% of industry-sponsored studies reflect no harm.
I didn’t learn that 95% of the people who created the recent USDA food guidelines for America had significant conflicts of interest with the food industry.
I did not learn that one billion pounds of synthetic pesticides are being sprayed on our foods every single year. 99% of the farmland in the United States is sprayed with synthetic pesticides, many from China and Germany, and these invisible, tasteless chemicals are strongly linked to autism, ADHD, sex hormone disruption, thyroid disease, sperm dysfunction, Alzheimer’s, dementia, birth defects, cancer, obesity, liver dysfunction, female infertility and more.
I did not learn that the eight billion tons of plastic that have been produced just in the last 100 years … are being broken down into microplastics that are now filling our food, our water, and we are now even inhaling them in our air, and that very recent research … tells us that now about 0.5% of our brains by weight are plastic.
I didn’t learn that there are more than 80,000 toxins that have entered our food, water, air, and homes by industry, many of which are banned in Europe, and they are known to alter our gene expression, alter our microbiome composition and the lining of our gut, and disrupt our hormones.
I didn’t learn that heavy metals like aluminum and lead are present in our food, our baby formula, personal care products, our soil, and many of the mandated medications like vaccines, and that these metals are neurotoxic and inflammatory.
I didn’t learn that the average American walks a paltry 3,500 steps per day even though we know, based on science and top journals, that simply walking 7,000 steps a day slashes by 40-60% our risk of Alzheimer’s, dementia, type 2 diabetes, cancer, and obesity.
I certainly did not learn that medical error and medications are the third-leading cause of death in the US. I didn’t learn that just five nights of sleep deprivation can induce full-blown pre-diabetes. I learned nothing about sleep, and we’re getting about 20% less sleep on average than we were 100 years ago.
I didn’t learn that American children are getting less time outdoors now than a maximum security prisoner, and on average, adults spend 93% of their time indoors, even though we know from the science that separation from sunlight destroys our circadian biology, and circadian biology dictated our cellular biology.
I didn’t learn that professional organizations that we get out practice guidelines from, like the American Diabetes Association and the American Academy of Pediatrics, have taken tens of millions of dollars from Coke, Cadbury, processed food companies and vaccine manufacturers like Moderna.
I didn’t learn that if you address these root causes that all lead to metabolic dysfunction and help patients change their food and lifestyle patterns … we could reverse the chronic disease crisis in America, save millions of lives and trillions of dollars in healthcare costs per year.
This is a spiritual crisis. We are choosing death over life, we are choosing darkness over light. We need a return to courage. We need a return to common sense and intuition. We need a return to awe for the sheer miraculousness of our lives. We need all hands on deck.”
Source: Sen. Ron Johnson’s Roundtable on “American Health and Nutrition: A Second Opinion” View: on X
“What they’re doing with the World Health Organization is one of the most breathtaking global power grabs we have seen in all of recorded human history. They are at this point transparently seeking the power to turn the WHO into not just like a global ministry of health or a global department of health and human services complete with an FDA, a CDC, HHS, all the different various divisions.
But when you look at how they define healthcare, when you look at how they define health emergencies, whether we’re looking at the one health where the health of humans is intimately intertwined with the climate and the grass and the animals and the ocean and all the rest of it, or when you, right, precisely, is one health, it is this integrated holistic view of health as something that encompasses every area of everything, right? And then the other side of this, which is that everything essentially is a public health emergency, as they’ve said publicly.
I was in Egypt and on the Arabian Peninsula at the last two climate summits where the head of the World Health Organization the CCP Operative dr. Tedros Ghebreyesus braces former politburo member of a mass murdering ethno-marxist terrorist organization called the Tigray People’s Liberation Front when he openly said that Climate change is a public health emergency. They’ve also said that racism is a public health emergency and gun violence is a public health emergency.
So If all of those things are public health emergencies, and they have told us that they are, every area of your life would then fall under the purview of this entity if it was able to usurp this power that it is seeking. They did take one big leap forward, no pun intended, with the adoption of some of the amendments to the international health regulations.
And Tedros has actually made perfectly clear that they intend to slam through this international pandemic treaty, accord, agreement. They’ve got different names. I think for technical legal reasons. They know they’re not going to get it through the US Senate, but it is a treaty. And they promise they’re going to do that either by the end of this year or at the very latest May of 2025. So they have not given up. They will not give up unless and until humanity says no.”
New Texas law could impact thousands of young people who want to change.
Potentially thousands of Texas children seeking to change their gender identity will no longer have access to puberty blockers, sterilization, and permanently disfiguring “gender-transition” surgeries in the state under a new law signed by Texas Gov. Gregg Abbott.
The Republican governor signed Senate Bill 14 on June 2, making the Lone Star State the most populous state to prohibit sex-change “treatments” for children.
The new law stands to be a major roadblock for advocates of transgender medicine.
Texas Children’s Hospital in Houston. (Courtesy of Texas Children’s Hospital via Google Maps)
It will stop the nation’s largest pediatric healthcare provider, Texas Children’s Hospital in Houston, from offering “gender-modification” procedures to minors.
And it will prohibit three more of the country’s largest pediatric hospitals from offering services to children who want to change their gender.
Both Texas Children’s Hospital, with 973 beds, and Children’s Medical Center of Dallas, with 490 beds, currently offer gender-altering services to youths.
Halting Surgeries in Texas
The new law just signed by Abbott bans surgeries that sterilize children by removing parts of their reproductive systems. It outlaws mastectomies for girls hoping to live more like boys.
It disallows the prescribing of drugs that induce temporary or permanent infertility, such as cross-sex hormones. And it prohibits removing any otherwise healthy or non-diseased body part.
The Lone Star State joins 17 other states now restricting “gender transitioning” for children. The Texas law will go into effect on Sept. 1.
Almost 30,000 Texas teens—from age 13 through 17—likely have a “gender identity” different from their biological sex, according to a study by the Williams Institute, part of the University of California, Los Angeles (UCLA) School of Law.
And nearly one in five people in the United States who identify as transgender are minors as young as 13, the study says.
Under the new law, children in Texas currently on hormones for gender dysphoria will have to be weaned off those drugs.
Police face pro-transgender protesters outside of Boston Children’s Hospital in Boston, Mass., on Sept. 18, 2022. (Joseph Prezioso/AFP via Getty Images)
Doctors who perform gender modification on children stand to lose their medical licenses in Texas. The bill gives the Texas attorney general the ability to enforce the law.
The Republican-led effort to pass SB 14—a priority for Lt. Gov. Dan Patrick, a Republican—met stiff resistance from Democrats as it was debated in May.
GOP advocates of the bill said cross-sex hormones, puberty blockers, and surgery could cause irrevocable health problems or sterility in children.
Their Democrat counterparts argued that the decision to put children on hormone treatment and surgery should be left to parents, their children, and doctors.
Journalist Chris Rufo, an outspoken opponent of “woke” gender ideology and gender modification for children, posted an undated internal emailfrom Texas Children’s Hospital CEO Mark Wallace on Twitter in May.
‘Immensely Heart-Wrenching’
In the email, Wallace announced an “immensely heart-wrenching” transition to modify “gender-affirming care” offered to children.
Protesters at Matt Walsh’s “Rally to End Child Mutilation” hold signs advocating for transgender rights in Nashville, Tenn., on Oct. 21, 2022. (Bobby Sanchez for The Epoch Times)
Action will be taken over the next few months to comply with the new law that will “prohibit procedures and prescription treatments for gender transitioning, gender reassignment, and gender dysphoria” for children, Wallace wrote.
He wrote that the hospital would “work with patients and their families to manage the discontinuation of hormone therapies or source appropriate care outside of Texas.”
And the hospital, he wrote, will “continue to offer psychosocial support and any form of care we can within the bounds of the law” through “this adversity.”
He said staff would “navigate these next steps together with grace, love, and compassion.”
Wallace wrote that he wanted to “remind everyone that our mission is to create a healthier future for all children.”
He wrote that “being unable to serve and support these children and families the way we have in the past is painful,” and that the hospital would “remain dedicated to educating and amplifying the importance of safe, high-quality transgender medicine programs.”
And he asked for support, empathy, and care for children, families, and “care teams who are deeply affected by this new legislation.” He wrote that he wanted to “reassure care teams” who “have devoted their lives to gender-affirming care” that they are “deeply valued.”
Texas lawmakers debated banning gender modification for children at the Capitol in Austin in May 2023. (Courtesy of the Texas Legislature)
Another large hospital, Children’s Medical Center of Dallas, will have to stop treating hundreds of minors with hormone “therapy.”
The hospital, part of the Children’s Health System of Texas, operates a gender clinic in conjunction with UT Southwestern Medical Center, also in Dallas.
The clinic, started by Dr. Ximena Lopez in 2014, is called the GENder Education and Care, Interdisciplinary Support (GENECIS) program.
Lopez, a pediatric endocrinologist, has said publicly that she will close her practice in July and move to California because of the new law.
State lawmakers, including Abbott and Attorney General Ken Paxton, have been pushing to ban transgender medical procedures for children for the past two years.
Paxton now has been replaced by an interim attorney general while he awaits a trial in the Texas Senate after being impeached by the Texas House.
Texas Gov. Greg Abbott speaks during a news conference in Austin, Texas, on March 15, 2023. (Brandon Bell/Getty Images)
Before his current problems, Paxton was part of a campaign to apply enough political pressure to hamstring GENECIS in November 2021, when the clinic was closed to new patients.
The clinic was allowed to continue seeing existing patients.
After Lopez filed a lawsuit in March 2022 seeking to fully reopen the clinic, a Dallas judge issued a temporary order, allowing the clinic to continue seeing new patients until the case could be settled in court.
A request for comment from Southwestern Medical Center on the status of the GENECIS clinic was not immediately returned.
Local news outlets reported that 100 families with children signed up for care as soon as the clinic reopened.
Do No Harm
Dr. Stanley Goldfarb, board chairman of Do No Harm. (Courtesy of Do No Harm)
Dr. Stanley Goldfarb is chairman of the board for Do No Harm, a group that fights “radical” ideologies in medicine.
Texas’ new law is significant because it affects large treatment centers for transgender youth, Goldfarb told The Epoch Times.
Children who are confused about their gender need mental health care instead of surgeries or hormones, Goldfarb said.
“The vast, vast majority of these children bring with them a tremendous burden of psychological difficulty,” he said.
“I hope [the hospitals] pivot to the right kind of care for these children.”
Some pediatric hospitals operate on the theory that the reason children with gender dysphoria have psychological problems is because they haven’t had a chance to change their gender, he said.
Once the children are allowed to transition to a different gender, advocates think the psychological problems experienced by these children will go away, he added.
But evidence from several studies suggests that the opposite happens, he said.
“The literature doesn’t show their psychological problems will go away.”
There can be little doubt that we are at war, except it’s not quite like in the movies. This war is unlike any others about which we learned in school where two opposed forces meet in a battlefield and fight it out until one side prevails. That kind of war is happening in Ukraine, but that’s only a part of the conflict that’s engulfed nearly all the rest of the world. It manifests in different and seemingly unrelated ways, but it is part of the same conflict.
Some analysts like to use the phrase “hybrid” or “asymmetrical” to describe it, by which they mean that in addition to shooting, the conflict has information, cultural, economic and financial dimensions. But I think that the war is still bigger than that: it is global and total – perhaps it should be called total global war. The “Trans Day of Vengeance” planned in Washington DC, is only the latest and weirdest part of it.
The clash of two systems
In his address to the World Economic Forum gathering in Davos in May 2022 George Soros explained that we are witnessing a clash between two models of governance. This was only slightly misleading: models don’t wage war on one another; it is the stakeholders in these models that are fighting. Soros characterized the two opposing sides as “open societies,” vs. “closed societies,” where open societies are liberal democracies that respect human rights, and closed societies are autocracies.
But Soros’s “open” societies are in fact oligarchies concealed behind faux democratic facades. To believe Soros, we’d have to accept that the trillionaire oligarchs in charge of open societies are die-hard defenders of democracy and human rights, willing to shed blood and treasure in their defense.
This war is as old as fractional reserve banking
But the notion that the conflict is between “two governance models” is not new: it is as old as the oldest forms of fractional reserve banking. Abraham Lincoln‘s chief economic advisor Henry C. Carey characterized it a bit better than George Soros. In his 1851 work, “The Harmony of Interests.” Carey wrote as follows:
“Two systems are before the world; the one looks to increasing the proportion of persons and of capital engaged in trade and transportation, and therefore to diminishing the proportion engaged in producing commodities with which to trade, with necessarily diminished return to the labour of all; while the other looks to increasing the proportion engaged in the work of production, and diminishing that engaged in trade and transportation, with increased return to all, giving the labourer good wages, and to the owner of capital good profits.
One looks to increasing the quantity of raw materials to be exported, and diminishing the inducements to imports of men, thus impoverishing both farmer and planter by throwing on them the burden of freight; while the other looks to increasing the import of men and diminishing the export of raw materials, thereby enriching both planter and farmer by relieving them from payment of freight.
One looks to giving the (products) of millions of acres of land and of the labour of millions of men for the (services) of hundreds of thousands of distant men; the other to bringing the distant men to consume on the land the products of the land, exchanging day’s labour for day’s labour.
One looks to compelling the farmers and planters of the Union to continue their contributions for the support of the fleets and the armies, the paupers, the nobles and the sovereigns of Europe; the other to enabling ourselves to apply the same means to the moral and intellectual improvement of the sovereigns of America.
One looks to the continuance of that freedom of trade which denies the principle of protection, yet doles it out as revenue duties; the other by extending the area of legitimate free trade by the establishment of perfect protection, followed by the annexation of individuals and communities, and ultimately by the abolition of customs-houses.
One looks to exporting men to occupy desert tracts, the sovereignty of which is obtained by aid of diplomacy or war; the other to increasing the value of an immense extent of vacant land by importing men by millions for their occupation.
One looks to the centralization of wealth and power in a great commercial city that shall rival the great cities of modern times which have been and are being supported by aid of contributions which have exhausted every nation subjected to them; the other to concentration, by aid of which a market shall be made upon the land for the products of the land, and the farmer and planter be enriched.
One looks to increasing the necessity of commerce; the other to increasing the power to maintain it.
One looks to underworking the Hindoo, and sinking the rest of the world to his level; the other to raising the standard of man throughout the world to our level.
One looks towards universal war; the other towards universal peace.
One is the English system; the other we may be proud to call the American system, for it is the only one ever devised the tendency of which was that of elevating while equalizing the condition of man throughout the world.”
Now, if you are like me, and perhaps you studied economics and history, you know about Adam Smith and John Maynard Keynes, but you probably never heard of Henry C. Carey. I am grateful to Cynthia Chung and Matthew Ehret for bringing Carey’s work to my attention through their invaluable research. If ever you read Carey’s biography, you might wonder why one of the most important economists of his age dropped out of the curriculum.
Well, the total global war is the reason. Namely, the proponents of the “open society” governance model would prefer it if you didn’t know about Henry Carey or about the American system which had turned the United States from a number of British Empire’s disjointed colonies into the world’s most prosperous and most powerful nation. In Lincoln’s days, the United States was known as a nation of readers, many of whom understood clearly what they were up against.
The rise of the United States in fact became such a threat to the British Empire that it orchestrated a civil war in order to break the Union into two smaller, weaker client states that could be set one against one another and kept weak and easily dominated. Empires do not suffer rivals and prefer that the earth be covered by uneducated and disorganized masses whose sole worth would be as a source of cheap, or preferably free labor used to extract their countries’ resource wealth and transfer it to “the nobles and sovereigns of Europe.” These would be the very stakeholders of George Soros’ open societies, who congregate in Davos and fantasize about turning the whole of humanity into a flock of “hackable animals” with no free will.
Even if the shooting war is raging in Ukraine, the United States remains the central battlefield in this total war. The people of the US are under a seemingly unrelated barrage of attacks that have escalated for several decades now and are almost too many to enumerate, but their effects include a sustained decline in living standards, progressive collapse of the nation’s infrastructure, loss of freedoms and permanent warfare. And yes, Americans are dying, only not exactly in trenches:
They already lost!
But the occult oligarchy behind the open societies has already lost their global war. They predicated their plans on achieving total domination of the whole world. The emergence of a multi-polar order entirely collapses their plans. How can you force everyone to rely on windmills and solar panels if your rivals are happily burning oil and gas and running their steel-producing furnaces? Without steel, you can’t build modern weapons. How can you coerce the “hackable animals” to subsist on insects if people in closed societies enjoy traditional foods? How do you force 7 or 8 billion people to take up your vaccines and carry vaccine passes if other nations opt for your rivals’ vaccines? That ship had sailed – it simply cannot be done.
Raising a new Iron Curtain
The only consolation prize available to the occult oligarchy now is to carve out a geopolitical block, break all ties with the closed societies and implement their plans within a new iron curtain. Then perhaps, the open societies could regroup and rebuild their military strength (not with solar panels) for another attempt at world domination in the future.
This new iron curtain would most likely encompass the UK, Canada, Australia, New Zealand and parts of continental Europe. But the block’s viability will depend on whether it can also include the United States which remains an extremely tough nut to crack. The uncontrolled migrations, attack on states’ rights, and the all-out assault of the Bill of Rights, including the periodic mass shootings, are all occult oligarchy’s attempts to crack it. It is all part of the total global war.
Like Henry Carey, those who understood the nature of this conflict knew that the ultimate showdown was coming. In addressing the American people, Ernesto Che Guevara invoked the coming clash: “I envy you. You North Americans are very lucky. You are fighting the most important fight of all – you live in the belly of the beast.” Che got many things wrong, but I believe he did get that part right.
Far and away the most common question I get from those who took one of the COVID-19 vaccines is: “how do I get this out of my body.” The mRNA and adenoviral DNA products were rolled out with no idea on how or when the body would ever breakdown the genetic code. The synthetic mRNA carried on lipid nanoparticles appears to be resistant to breakdown by human ribonucleases by design so the product would be long-lasting and produce the protein product of interest for a considerable time period. This would be an advantage for a normal human protein being replaced in a rare genetic deficiency state (e.g. alpha galactosidase in Fabry’s disease). However, it is a big problem when the protein is the pathogenic SARS-CoV-2 Spike. The adenoviral DNA (Janssen) should be broken down by deoxyribonuclease, however this has not be exhaustively studied.
This leaves dissolution of Spike protein as a therapeutic goal for the vaccine injured. With the respiratory infection, Spike is processed and activated by cellular proteases including transmembrane serine protein 2 (TMPRSS2), cathepsin, and furin. With vaccination, these systems may be avoided by systemic administration and production of Spike protein within cells. As a result, the pathogenesis of vaccine injury syndromes is believed to be driven by accumulation of Spike protein in cells, tissues, and organs.
Nattokinase is an enzyme is produced by fermenting soybeans with bacteria Bacillus subtilis var. natto and has been available as an oral supplement. It degrades fibrinogen, factor VII, cytokines, and factor VIII and has been studied for its cardiovascular benefits. Out of all the available therapies I have used in my practice and among all the proposed detoxification agents, I believe nattokinase and related peptides hold the greatest promise for patients at this time.
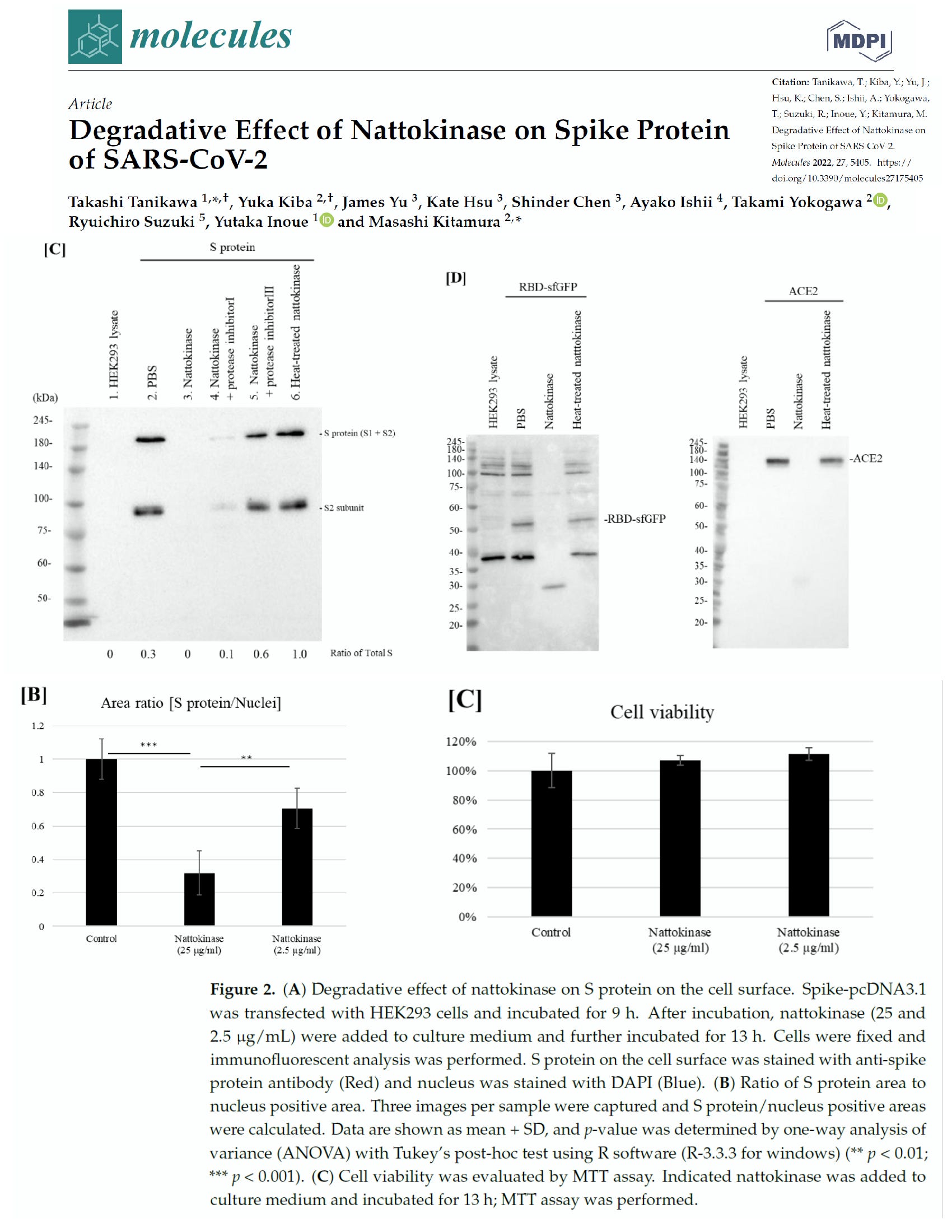
Tanikawa et al examined the effect of nattokinase on the Spike protein of SARS-CoV-2. In the first experiment they demonstrated that Spike was degraded in a time and dose dependent manner in a cell lysate preparation that could be analogous to a vaccine recipient. The second experiment demonstrated that nattokinase degraded the Spike protein in SARS-CoV-2 infected cells. This reproduced a similar study done by Oba and colleagues in 2021.
Tanikawa T, Kiba Y, Yu J, Hsu K, Chen S, Ishii A, Yokogawa T, Suzuki R, Inoue Y, Kitamura M. Degradative Effect of Nattokinase on Spike Protein of SARS-CoV-2. Molecules. 2022 Aug 24;27(17):5405. doi: 10.3390/molecules27175405. PMID: 36080170; PMCID: PMC9458005.
Nattokinase is dosed in fibrinolytic units (FU) per gram and can vary according to purity. Kurosawa and colleagues have shown in humans that after a single oral dose of 2000 FU D-dimer concentrations at 6, and 8 hours, and blood fibrin/fibrinogen degradation products at 4 hours after administration elevated significantly (p < 0.05, respectively). Thus an empiric starting dose could be 2000 FU twice a day. Full pharmacokinetic and pharmacodynamic studies have not been completed, but several years of market use as an over-the-counter supplement suggests nattokinase is safe with the main caveat being excessive bleeding and cautions with concurrent antiplatelet and anticoagulant drugs.
Based on these findings, nattokinase and similar products such as serrapeptase should undergo well-funded, accelerated preclinical and clinical development programs. The issue at hand is the urgency of time, similar to that with SARS-CoV-2 infection and empiric early therapy. It will take up to 20 years to have a fully developed pharmaceutical profile to characterize the safety and efficacy of nattokinase in the treatment of vaccine injury and post-COVID syndromes. Large number of people are sick now and many believe empiric treatment is justified given sufficiently low risk of side effects and potentially high reward. My recommendation is to discuss this with your doctor or seek a specialist in holistic or naturopathic medicine who is experienced with the safety profile of nattokinase in a range of applications.
If you find “Courageous Discourse” enjoyable and useful to your endeavors, please subscribe as a paying or founder member to support our efforts in helping you engage in these discussions with family, friends, and your extended circles.
Source:Courageous Discourse™ with Dr. Peter McCullough & John Leake is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Dr. Peter McCullough joins Alex Jones live in studio to give his powerful presentation on the COVID virus, its mutations, and the mRNA gene therapy/viral vector injections.
Segment 1 – Introduction
In this segment Dr. Peter McCullough touches on the public policy decisions in response to Covid-19 that have resulted in mass death, and the current international lawsuits alleging intentional crimes against humanity. The Doctor goes onto provide a big picture analysis of C19’s origins at the Wuhan Lab, and distinctions between it’s variants. This segment provides the basis for the detailed presentations that follow including: facts about the viral lifecycle, Euler’s Ratchet, the importance of early treatment, Omicron vs Delta, confirmation that no test currently exists to identify variant identity, and finally citations from the study conducted on American loss of life due to the vaccines.
Segment 2 – The Great Gamble of C19 Vaccine Development
In the second part of Dr. McCullough’s InfoWars interview contrary to CDC/NIH guidelines the Doctor extols the urgent need for early ambulatory therapy for successful Covid-19 treatment. Dr. McCullough prefaces the discussion of experimental mRNA and adenovirus injections with review of an article titled, “The Great Gamble of C19 Vaccine Development.” This sets the stage for a deep dive into the origins of the C19 Spike Protein, and its mechanism of action. The segment culminates in corroboration of the Whuhan Lab theory, and a detailed explanation how vaccine damage occurs, and the tissues affected.
Segment 3- Medical Censorship & Countervailing Evidence
Dr. McCullough describes the attacks being waged on members of the medical community who publish examinations of the empirical evidence demonstrating Covid-19 vaccine damage. This includes an analysis of VAERS data showing disproportionate instances of myocarditis among men of all ages, plus a study using census data revealing up to 180,000 American deaths linked to the vaccine, making it a bigger killer than the illness. Finally, Dr. McCullough exposes the Regulatory Malfeasance occurring as CNN diabolically attempts to seduce young children to take the deadly vaccines through promotions running on Sesame Street.
A current lawsuit is challenging the secrecy of Pfizer’s vaccine trial data. Dr. Peter McCullough is one of the lead experts tasked with reviewing the data should the suit prevail. Currently, the fact pattern demonstrates zero transparency between the US Government and Pfizer. What are they hiding? The first priority is to “Do no harm” and safety is valued higher than efficacy, but Pfizer is attempting to seal all trial data for 70 years making product safety evaluations nearly impossible, while the Government is failing to conduct reviews according to statutory and historical measures. Dr. Peter McCullough advises the audience on the best way to stay healthy.
Dr. McCullough examines a recent study involving 780,000 VA Veterans. This and 22 other studies show waning vaccine efficacy over 3-6 months for all vaccines against all variants. Statistically this evidence demonstrates just a 1% mortality benefit, without addressing adverse events in adults, and young people geting no medical benefits from Covid-19 vaccination. With the waning efficacy, what does this mean going forward? Dr. Peter McCullough and Alex Jones predict increasing vaccine frequency tied to travel, work, etc. With Pfizer knowing about 1000’s of deaths following vaccination, is this part of a depopulation agenda?
The segment begins in review of the timeline and development of the Covid-19 pandemic including the well documented simulations preceding the outbreak that lead many to believe we are experiencing a well planned and orchestrated crisis.
Dr. McCullough reveals the genomic sequencing of the Omicron variant, which is unique from all previous strains of Covid. Omicron differs across 26 mutations occurring at the Receptor Binding Domain for ACE2 receptor sites, making this variant much less invasive than its predecessors. Dr. McCullough notes the presence of insertions in the Omicron genetic code, which are distinct from mutations, and could possibly indicate evidence of engineering.
Dr. McCullough also dispels the false claim that Omicron should be blamed on the unvaccinated, citing a study from Denmark showing 79% of Omicron infections occurring in fully vaccinated patients.
Alex Jones and Dr. McCullough discuss the war being waged against honest medical professionals attempting to save lives by revealing disastrous public policy measures in response to Covid-19. Examples include forced vaccination policies within hospitals like Houston Methodist, that have aggressively coerced staff to take the vaccination or face termination of employment. The result is these institutions are now facing shortages due to attrition of staff that resist such measures, and loss of staff due to high infection rates despite nearly 100% vaccination. The Doctor also touches on reactivation diseases resulting from immunosuppression, durability of immunity, and a pattern of the Government blocking effective therapeutics in favor of deadly vaccines.
Topics include federal monoclonal rationing, and CDC exoneration of unvaccinated as causing the pandemic by their own statistics. Dr. McCullough breaks down effective Early Outpatient Treatment Protocol consisting of: 1) Precautionary principle – mass casualty event, 2) Comprehensive evidence signalling, 3) Acceptable safety, and 4) Drugs in combination. Gold standard randomized trials indicate viracidal treatments with Iodine, H2O2, Colloidal Silver, and 03 are highly effective in stopping viral replication within the nasal passage.
Top Scientists call on the World Health Organization to shut down vaccinations against Omicron. Dr. McCullough describes the case for crimes against humanity, and issues an optimistic message for humanity.
Sovereign’s Handbook by Johnny Liberty (30th Anniversary Edition) (3-Volume Printed, Bound Book or PDF)
A three-volume, 750+ page tome with an extensive update of the renowned underground classic ~ the Global Sovereign’s Handbook. Still after all these years, this is the most comprehensive book on sovereignty, economics, law, power structures and history ever written. Served as the primary research behind the best-selling Global One Audio Course. Available Now!
Dawning of the Corona Age: Navigating the Pandemic by Johnny Freedom (3rd Edition) (Printed, Bound Book or PDF)
This comprehensive book, goes far beyond the immediate impact of the “pandemic”, but, along with the reader, imagines how our human world may be altered, both positively and negatively, long into an uncertain future. Available Now!