For over two decades, we have tirelessly advocated for two foundational pillars of true health freedom: nutritious, unadulterated food and a rational, risk-aware vaccine schedule. We often wondered if meaningful, systemic change was possible against the entrenched powers of Big Pharma and Big Agra. Today, thanks to the decisive leadership of President Donald J. Trump, that change is not just possible—it is the official policy of the United States government. By appointing Robert F. Kennedy Jr. as Secretary of Health and Human Services and giving him a clear mandate to dismantle the deep-state bureaucracy, President Trump has turned our long-held principles into national action. 😊
While other administrations talked about “draining the swamp,” when it comes to these two pillars, President Trump is authorizing the machinery to do it, and the Trump-Kennedy partnership is waging a decisive, domestic campaign for the sovereignty of the American body. Where past leaders turned a blind eye to corporate capture, this administration is seizing the moment to liberate our children’s bodies and our families’ plates. This is more than reform; it is a peaceful revolution in public health, made possible by a President who understands that true national strength begins with the health of its people.
The Real Food Pyramid: Reclaiming Our Nutritional Heritage
For generations, the USDA’s food pyramid stood as a monument to misguided science and Big Agra influence, promoting processed grains and sugars that fueled a pandemic of diabetes, obesity, and heart disease. Secretary Kennedy, in one of his first major acts, dismantled this corrupt edifice and introduced the Real Food Pyramid.
As you can see from the image above, taken from RealFood.gov, the previous food pyramid was upside down! RFK just turned it right side up! 😊 The new guidelines emphasize eating real food, defined as minimally processed foods “prepared with few ingredients and without added sugars, industrial oils, artificial flavors, or preservatives.”
This isn’t a minor adjustment; it’s a philosophical renaissance. What has been announced is nothing less than the structural and symbolic flipping of the pyramid. For decades, this inverted logic was an instrument of captured interests, placing refined carbohydrates at the base, labeling industrial seed oils as “heart healthy,” and pushing protein and traditional fats to the margins.
This created a vicious economic flywheel: weaponized food → metabolic dysfunction → chronic disease → sick-care dependency → lifelong pharmaceutical drugs to manage symptoms. Basically, a closed loop of profit and sickness.
The new pyramid emphasizes:
Whole, nutrient-dense foods from regenerative and organic agriculture.
Healthy, ancestral fats over industrially processed seed oils.
Protein quality, prioritizing pasture-raised and wild-caught sources.
By flipping the pyramid, this administration is breaking a control architecture that has quietly governed public health for half a century. It is centering the foods humanity has always (until recently) eaten: high-quality protein, natural fats (including traditionally demonized saturated fats), and whole foods in their intact forms. It is finally displacing the industrial seed oils, ultra-processed carbohydrates, and food-like substances engineered for addiction and profit.
This isn’t nostalgia; it’s biological realism. Human physiology thrives on nutrient density and fats that stabilize our biology, and food itself contains gene-regulatory exosomes that literally “talk” to our cells. This correction interrupts the very feedback loop that feeds both the chronic disease epidemic and the drug industries built to manage it. When you flip the pyramid, you don’t just change what people eat—you change who benefits.
This policy directly aligns with the principles we’ve championed for years: that food is medicine, and that a corrupted food supply is a primary driver of chronic disease. At a White House press briefing, Kennedy called the changes the “most significant reset of federal nutrition policy in history.”
Kennedy said: “These guidelines replace corporate-driven assumptions with common-sense goals and gold-standard scientific integrity. These new guidelines will revolutionize our nation’s food culture and make America healthy again… For decades, Americans have grown sicker while healthcare costs have soared. The reason is clear: the hard truth is that our government has been lying to us to protect corporate profit-taking, telling us that these food-like substances were beneficial to public health… Federal policy promoted and subsidized highly processed foods and refined carbohydrates and turned a blind eye to the disastrous consequences. Today, the lies stop.”
This historic shift is being translated into operational reality across the government, including the U.S. Public Health Service Commissioned Corps and military health services. You cannot sustain national security, readiness, or operational capacity on ultra-processed food. A nation cannot be strong if those sworn to defend it are metabolically compromised. This is what it looks like when policy confronts the chronic disease epidemic at its root.
Kennedy’s move boldly rejects the lobbyist playbook and realigns federal policy with peer-reviewed science on metabolic health. This is a victory for every family farmer, every conscious consumer, and every parent seeking to nourish their children properly, a sentiment echoed in discussions of his broader plan to combat childhood chronic diseases.
A guideline is a blueprint. The real work is implementation: federal procurement shifting toward real food, school lunch reform accelerating, and medical institutions being forced by evidence to catch up. This is the beginning of a national reorientation away from symptom-management and toward true prevention. We now have a historic invitation: to eat real food, support the farmers who steward life, and build meals that restore metabolism and resilience. The tide is turning.
Restoring Sanity and Safety to Childhood Vaccines
For decades, the U.S. childhood immunization schedule has been presented not as a set of clinical recommendations, but as a non-negotiable mandate. This rigid, “one-size-fits-all” model was predicated on a flawed premise: that public health is best served by removing physician judgment and patient context from the equation. The truth is that this system was corrupted by perverse financial incentives that placed profit above individual care.
Previously, pediatricians were financially incentivized to meet aggressive vaccination quotas. Initiatives like the “Combo 10” benchmark—where practices received bonuses of $400 per child from insurers like Blue Cross Blue Shield for achieving a 63% vaccination rate across their entire patient base—transformed doctors from caregivers into commission-driven sales agents. Below is a video of RFK, Jr. and Dr. Sherri Tenpenny from our 2023 docu-series – REMEDY – elaborating on this topic.
These coercive pay-for-performance schemes are now being systematically dismantled by Kennedy’s HHS, which has directed the Centers for Medicare & Medicaid Services (CMS) to end financial incentives tied solely to vaccination rates.
The message was clear: the system valued blanket compliance over careful, individualized medical evaluation. As Kennedy stated on video in 2025, “Doctors are being paid to vaccinate, not to evaluate. They’re pressured to follow the money, not the science.”
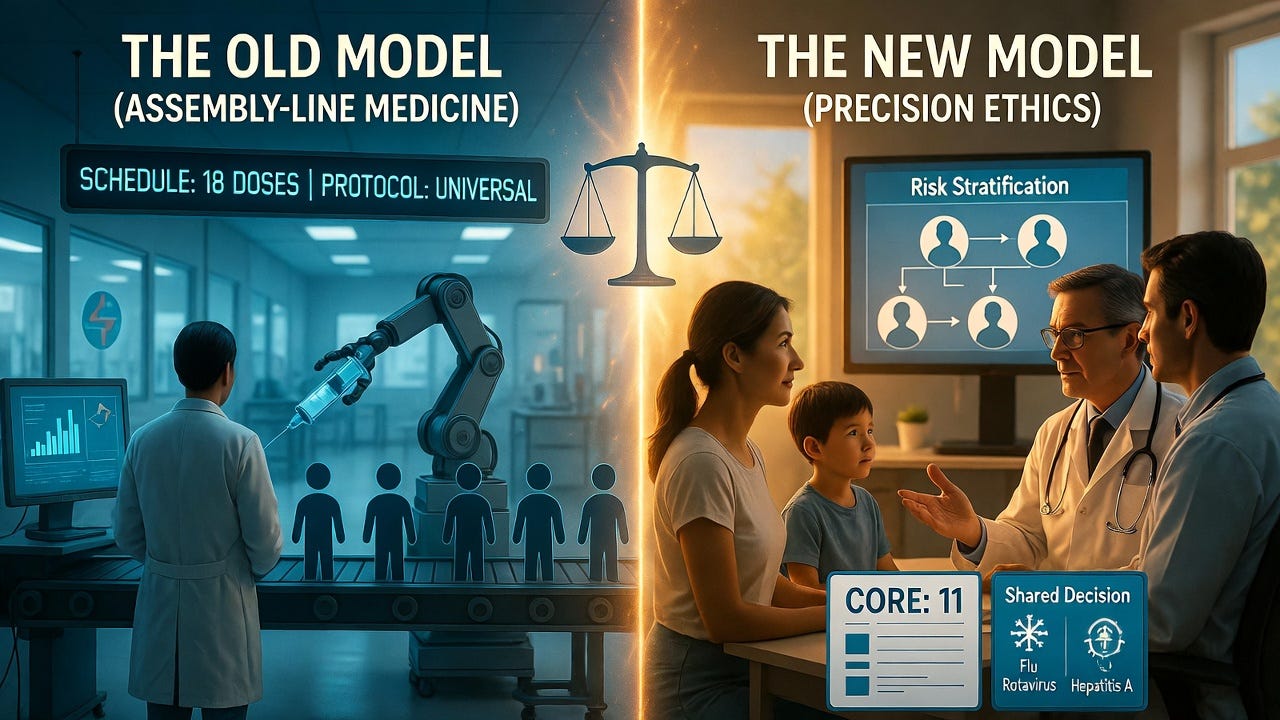
The reforms enacted in January 2026 under the leadership of Robert F. Kennedy Jr. at the CDC represent a historic correction. This was not a reckless reduction but a scientifically grounded restoration of medical ethics. The schedule was revised from a bloated 18 universally recommended doses down to a core 11, moving vaccines for influenza, rotavirus, hepatitis A, and certain meningitis strains into a category of “shared clinical decision-making.” This shift explicitly gives parents a meaningful say in whether their child receives certain vaccines, requiring a conversation about risks and benefits rather than an automatic administration.
This long-overdue correction is grounded in a foundational, yet inconvenient, epidemiological truth: population risk is heterogeneous, not homogeneous. The reformed schedule finally moves away from the pseudoscientific, assembly-line model of medicine and toward a risk-stratified approach. It restores the physician’s role by empowering them to utilize clinical discretion—considering a child’s individual immune status, genetic predispositions, and actual environmental risk—rather than functioning as a rubber stamp for a coercive, profit-maximizing protocol. Re-categorizing vaccines for pathogens like COVID-19, RSV, and Hepatitis B to “high-risk only” status isn’t a reduction in care; it’s the precise application of medicine, reserving medical interventions for those who actually stand to benefit from them. This is how science is supposed to work, outside the boardrooms of pharmaceutical manufacturers.
The subsequent exodus of career bureaucrats from the CDC is not brain drain; it’s a parasite purge. Their resignations are a de facto admission that the agency’s old operating principle—serving as a marketing arm for Big Pharma—is no longer tenable. Good riddance. The institution can now be rebuilt on the pillars it long ago abandoned: rigorous, hypothesis-driven science, transparent and quantifiable risk-benefit disclosures, and the non-negotiable ethical standard of informed consent.
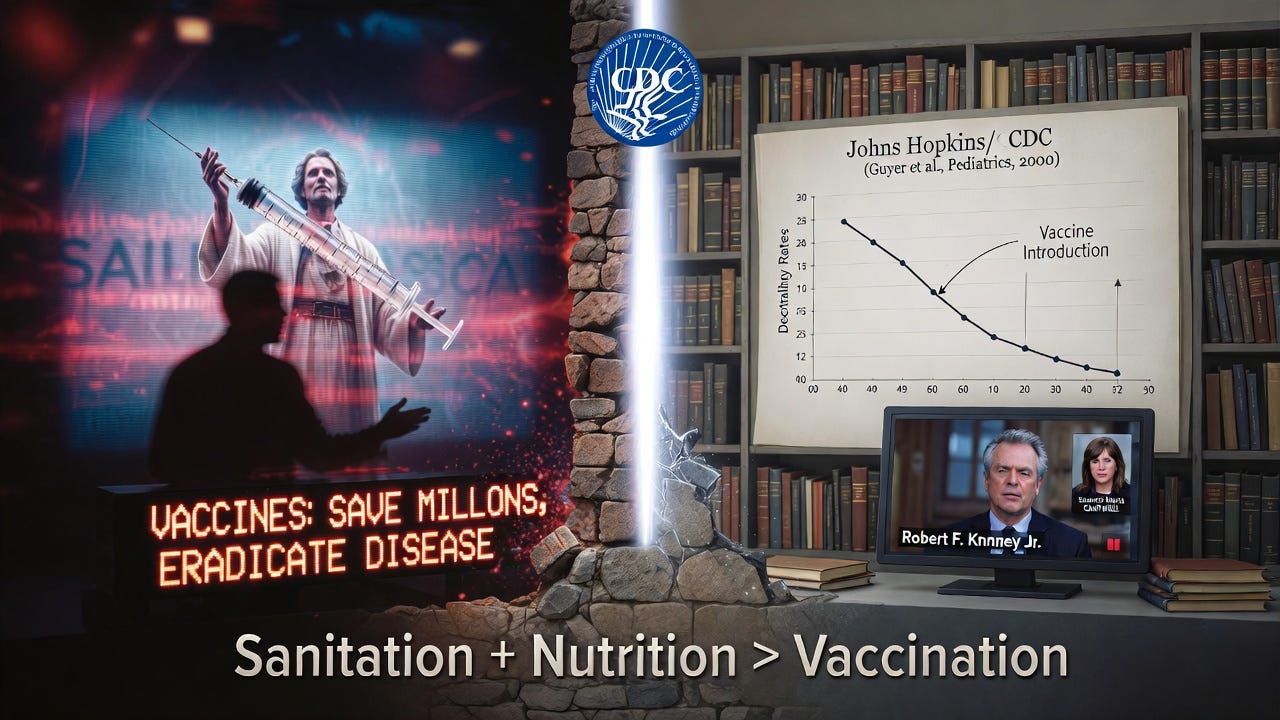
This reform exposes the central, vacuous mantra of the pro-mandate lobby. We are incessantly lectured by those with a vested financial or ideological interest—often with the scientific depth of a cable news chyron—that “vaccines save millions of lives and eradicate disease.” One such devotee of this faith-based immunology was Senator Maria Cantwell (D-Wash.), whose simplistic pronouncements on the matter Kennedy dismantled with factual precision in a rebuttal that should be mandatory viewing.
The historical data, curiously absent from their talking points, undermines their entire narrative. Consider the CDC’s own investment in truth: a study funded by the CDC and conducted by researchers at Johns Hopkins analyzed a century of U.S. mortality data. Its conclusion was empirically clear and devastating to the salvation myth of vaccination: nearly 90% of the decline in mortality from common infectious diseases occurred before the introduction of their corresponding vaccines.
The dramatic reduction was attributable to improved sanitation, nutrition, and living standards—facts the “vaccines or death” evangelists conveniently ignore. The 2026 reforms finally begin to align policy with this uncontested historical record, prioritizing real public health over pharmaceutical evangelism.
Transformative, Decisive Leadership
Robert F. Kennedy Jr. is demonstrating what transformative leadership looks like, and he is doing so with the essential backing of a President willing to break the old molds. President Trump, by supporting this agenda, has taken the very issues patriots have long held sacred—medical freedom, environmental purity, and untainted food—and created the political space for them to become national policy. This is not partisan politics; it is the restoration of foundational American values: liberty, informed consent, and sovereignty over our own bodies.
These historic accomplishments, made possible under this administration, provide a tangible, powerful reason for hope. They are a blueprint for a stronger, healthier, and more independent America. This is the work we voted for. This is the promise of “America First” applied to the most personal frontier of all: our health. Let us celebrate these victories, support the courageous leaders making them possible, and continue this essential journey toward reclaiming our nation’s vitality from the ground up.
President Trump acknowledges that Republicans hate the COVID vaccine, and that he is open to admitting the shots were damaging, but is waiting for long term studies to be released in 2025.
“I think they’re doing studies on the vaccines that we’re gonna find out. And it’ll come out one way or the other. But I really had a mandate to get vaccines done. And I got ’em done very quickly in record time. The Democrats love it. You know, the Democrats love it and the Republicans don’t. It’s very interesting.”
In this stellar interview with Full Measure host Sharyl Attkisson, who bravely pointed out that not only do the shots NOT “prevent infection, illness, or transmission” but have “very potentially serious side effects,” President Trump said he thought he did a great job handling the pandemic.
“The vaccines. They love it. I have a friend of mine who said to me, ‘why don’t you talk about the vaccine, what you did with the vaxx.’ He’s a Democrat, but I’m sure he voted for me. He said, ‘what you did was the most incredible thing that any president has ever done. You’ve saved hundreds of millions of lives all over the world.’ And this was just recently very smart guy. He said, ‘I don’t understand why you don’t talk about it.’ And I don’t talk about it.
But if you go to Pfizer, if you go to some of these companies, they have charts and they have all sorts of statistics. And I say, ‘why don’t you release those statistics? Let people know.’ But I don’t talk about it. I can say this, the Democrats would love to claim it. The Republicans don’t want to claim it. But it’ll be determined, I’d say over the next 12 months. I say this in terms of overall, I think I did an amazing job with Covid. I never got the credit for it. Remember that more people died under Biden-Harris than died under Trump. And they had a much easier time because when it came in here, nobody knew what it was. It came from the Wuhan labs, which I always said. But nobody really knew what it was, where it came from. Nothing. They knew nothing.”
Sharyl is an example of the few, ethical, smart, and dedicated journalists left on the national stage, who put the truth over access and fame.
A controversial forecast by Deagel, a global intelligence and consulting firm, recently gained attention for its startling prediction of a significant depopulation event by 2025. While initially dismissed as a speculative estimation, current events and emerging trends have led many to question whether there may be more to Deagel’s forecast than meets the eye.
Recent reports from the Governments of the USA, Canada, Australia, New Zealand, the UK, and various European countries have brought forth troubling revelations, among which is confirmation of a staggering number of excess deaths, reaching over two million since the mass roll-out of Covid-19 injections.
A troubling 120,000 excess deaths have also been recorded among the USA’s infants, children and young adults as of week 40 of 2022, and a curious rise in excess deaths among children across Europe has been recorded ever since the European Medicines Agency (EMA) extended the Emergency Use Authorization (EUA) of the Pfizer Covid-19 injection to children in the middle of 2021.
With further Government figures confirming mortality rates are highest among the vaccinated in every single age group per 100,000 population, serious questions are now being raised about the accuracy and potential truth behind Deagel’s apocalyptic depopulation predictions.
What is Deagel? The Deagel corporation is a minor branch of US military intelligence, one of the many secretive organizations which collect data for high-level decision-making purposes and prepares confidential briefing documents for agencies like the National Security Agency, the United Nations, and the World Bank.
It is known to have contributed to a Stratfor report on North Korea. With this kind of pedigree, Deagel should be seen as a legitimate player in the intelligence community and not merely a disinformation asset.
This means its population predictions for 2025, as well as its industrial output predictions on a nation-by-nation basis, are not mere fantasy but instead based on strategic assumptions which are shared and well understood by other players in the intelligence community.
What has Deagel Predicted? Deagel.com’s [infamous] 2025 forecast was removed from their website sometime in 2020. However, thanks to the Wayback Machine / Internet Archive, we are able to view the original predictions before discovered by critical thinkers.
Deagel predicted in 2020 that the United Kingdom would see its population decline by 77.1% by the year 2025. Deagel predicted in 2020 that the United States would see its population decline by 68.5 % by the year 2025. Read more…
Technology expert Michael Rectenwald, Ph.D., told The Defender that, under the guise of preserving freedom, a digital passport system “means restraints on movement and living for the unvaccinated and forced vaccination to participate in life.”
The World Health Organization (WHO) and the European Commission — the executive branch of the European Union (EU) — on Monday launched a “landmark digital health partnership” marking the beginning of the WHO Global Digital Health Certification Network (GDHCN) to promote a global interoperable digital vaccine passport.
Beginning this month, the WHO will adopt the EU’s system of digital COVID-19 certification “to establish a global system that will help facilitate global mobility and protect citizens across the world from on-going and future health threats, including pandemics,” according to Monday’s announcements by the WHO and the European Commission.
The WHO and European Commission claim the GDHCN initiative, which has been in the works since 2021, “will develop a wide range of digital products to deliver better health for all.”
The organizations said the WHO will not collect individuals’ personal data via these digital passports — stating that such data collection “would continue to be the exclusive domain of governments.”
WHO Director-General Tedros Adhanom Ghebreyesus lauded the new agreement:
“Building on the EU’s highly successful digital certification network, WHO aims to offer all WHO Member States access to an open-source digital health tool, which is based on the principles of equity, innovation, transparency and data protection and privacy.
“New digital health products in development aim to help people everywhere receive quality health services quickly and more effectively.”
However, experts who spoke with The Defender said the ramifications of such a system for human liberty and freedom of movement raised concerns.
Independent journalist James Roguski told The Defender the WHO is not waiting for a successful conclusion of these negotiations in order to implement initiatives such as a global digital vaccine passport. He said:
“The announcement by the WHO and the European Commission regarding the launch of their digital health partnership was hardly a surprise. Over a month ago, the WHO quietly published that they were working on ‘operationalizing’ the very things that were being ‘negotiated.’
“This is just one example that clearly shows that the super-secret ‘negotiations’ regarding the International Health Regulations (IHR) are a charade.”
Michael Rectenwald, Ph.D., author of “Google Archipelago: The Digital Gulag and the Simulation of Freedom,” told The Defender that, under the guise of preserving freedom, a digital passport system “means restraints on movement and living for the unvaccinated and forced vaccination to participate in life.”
The announcement of the WHO-European Commission collaboration came just days after the conclusion of the WHO’s annual World Health Assembly (WHA).
While the pandemic treaty and IHR amendments were not finalized at this year’s meeting, high-level WHO officials warned of the risk of a future pandemic and spread of a deadly “Disease X,” and expressed the need to “restrict personal liberties” during a future health emergency.
The EU has been a strong proponent of digital vaccine passports, first launched for its member states in late 2020 — concurrent with the introduction of the COVID-19 vaccines — under the name “Green Pass.” The EU’s experience with the digital passes is noted in Monday’s announcement, which states:
“One of the key elements in the European Union’s work against the COVID-19 pandemic has been digital COVID-19 certificates. To facilitate free movement within its borders, the EU swiftly established interoperable COVID-19 certificates.
“Based on open-source technologies and standards it allowed also for the connection of non-EU countries that issue certificates … becoming the most widely used solution around the world.”
Roguski told The Defender the EU also was among the strongest proponents of vaccine passports during ongoing negotiations for the WHO’s “pandemic treaty” and amendments to the IHR.
“They really want the global digital health certificate,” Roguski told The Defender in March. “Primarily, that’s coming from the European Union.”
‘Pandemic passports a death sentence for millions’
According to Roguski, the EU, during negotiations for the IHR amendments, put forth proposals that seek to “‘normalize’ the implementation of a global digital health certificate.”
The Czech Republic called for Passenger Locator Forms “containing information concerning traveller’s destination,” preferably in digital form, for the purpose of contact tracing.
They also proposed that the WHO’s Health Assembly “may adopt, in cooperation with the International Civil Aviation Organization [ICAO] … and other relevant organisations, the requirements that documents in digital or paper form shall fulfill with regard to interoperability of information technology platforms, technical requirements of health documents, as well as safeguards to reduce the risk of abuse and falsification.”
The Czech Republic and the EU proposed documentation not just for vaccination, but “test certificates and recovery certificates” in cases “where a vaccine or prophylaxis has not yet been made available for a disease in respect of which a public health emergency of international concernhas been declared.”
Plans for the WHO’s GDHCN have been in the works since at least August 2021, when the WHO released a document titled “Digital documentation of COVID-19 certificates: vaccination status: technical specifications and implementation guidance, 27 August 2021.”
“The Secretariat has developed SMART (Standards-based, Machine-readable, Adaptive, Requirements-based, and Testable) Guidelines on the digital documentation of COVID-19 certificates, comprising recommendations on the data, digital functionality, ethics, and trust architecture needed to ensure the interoperability of immunization and health records globally.”
The WHO also announced the successful completion of a “technical feasibility study for establishing a federated global trust network, which tested the ability to interoperate the health content and trust networks across existing regional efforts.”
EU officials have frequently praised themselves over the launch of the bloc’s “Green Pass,” touting how individuals’ privacy would be protected on the app. The introduction of the “Green Pass” was accompanied by statements by European Commission President Ursula von der Leyen calling for a “discussion” on mandatory vaccinations in the EU.
One of the EU’s stated priorities as part of its 2019-2024 five-year plan is to create a “Digital Identity for all Europeans.” Namely, each EU citizen and resident would have access to a “personal digital wallet,” which would include national ID cards, birth and medical certificates, and drivers’ licenses.
These proposals and initiatives appear to be closely aligned with the United Nations’ Sustainable Development Goals (SDGs), and in particular, Target 16.9, which calls for the provision of a digital legal identity for all, including newborns, by 2030.
Tedros said the SDGs are “our north star,” while addressing this year’s WHA.
Rectenwald called “pandemic passports” a “death sentence for millions.” He told The Defender:
“Despite the studies demonstrating that vaccines to curb pandemics have been deadly and useless, the WHO is doubling down on vaccine mandates.
“Pandemic passports equal a death sentence for millions and the abrogation of rights for the non-compliant. The WHO should be stopped before it completes the construction of a global totalitarian system.”
Far and away the most common question I get from those who took one of the COVID-19 vaccines is: “how do I get this out of my body.” The mRNA and adenoviral DNA products were rolled out with no idea on how or when the body would ever breakdown the genetic code. The synthetic mRNA carried on lipid nanoparticles appears to be resistant to breakdown by human ribonucleases by design so the product would be long-lasting and produce the protein product of interest for a considerable time period. This would be an advantage for a normal human protein being replaced in a rare genetic deficiency state (e.g. alpha galactosidase in Fabry’s disease). However, it is a big problem when the protein is the pathogenic SARS-CoV-2 Spike. The adenoviral DNA (Janssen) should be broken down by deoxyribonuclease, however this has not be exhaustively studied.
This leaves dissolution of Spike protein as a therapeutic goal for the vaccine injured. With the respiratory infection, Spike is processed and activated by cellular proteases including transmembrane serine protein 2 (TMPRSS2), cathepsin, and furin. With vaccination, these systems may be avoided by systemic administration and production of Spike protein within cells. As a result, the pathogenesis of vaccine injury syndromes is believed to be driven by accumulation of Spike protein in cells, tissues, and organs.
Nattokinase is an enzyme is produced by fermenting soybeans with bacteria Bacillus subtilis var. natto and has been available as an oral supplement. It degrades fibrinogen, factor VII, cytokines, and factor VIII and has been studied for its cardiovascular benefits. Out of all the available therapies I have used in my practice and among all the proposed detoxification agents, I believe nattokinase and related peptides hold the greatest promise for patients at this time.
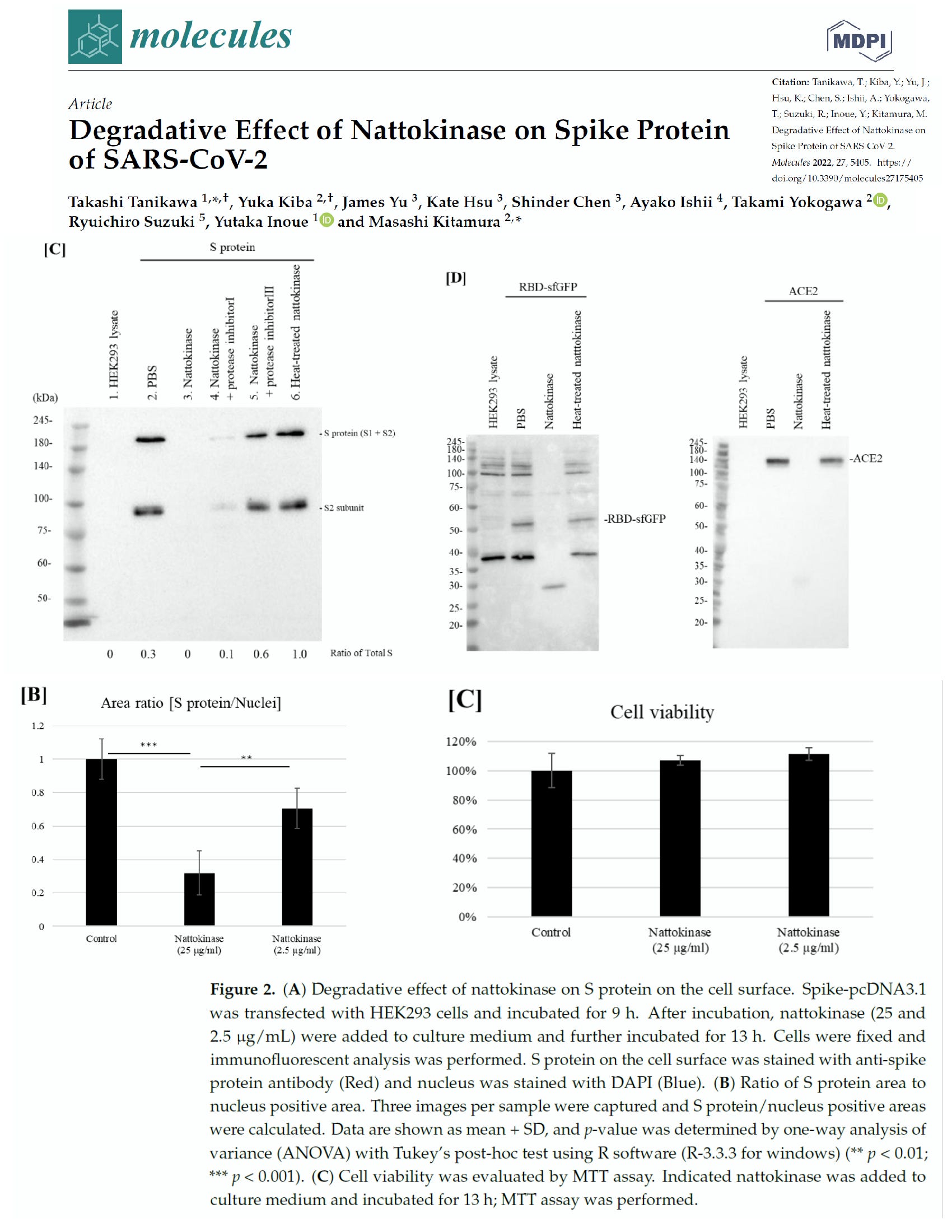
Tanikawa et al examined the effect of nattokinase on the Spike protein of SARS-CoV-2. In the first experiment they demonstrated that Spike was degraded in a time and dose dependent manner in a cell lysate preparation that could be analogous to a vaccine recipient. The second experiment demonstrated that nattokinase degraded the Spike protein in SARS-CoV-2 infected cells. This reproduced a similar study done by Oba and colleagues in 2021.
Tanikawa T, Kiba Y, Yu J, Hsu K, Chen S, Ishii A, Yokogawa T, Suzuki R, Inoue Y, Kitamura M. Degradative Effect of Nattokinase on Spike Protein of SARS-CoV-2. Molecules. 2022 Aug 24;27(17):5405. doi: 10.3390/molecules27175405. PMID: 36080170; PMCID: PMC9458005.
Nattokinase is dosed in fibrinolytic units (FU) per gram and can vary according to purity. Kurosawa and colleagues have shown in humans that after a single oral dose of 2000 FU D-dimer concentrations at 6, and 8 hours, and blood fibrin/fibrinogen degradation products at 4 hours after administration elevated significantly (p < 0.05, respectively). Thus an empiric starting dose could be 2000 FU twice a day. Full pharmacokinetic and pharmacodynamic studies have not been completed, but several years of market use as an over-the-counter supplement suggests nattokinase is safe with the main caveat being excessive bleeding and cautions with concurrent antiplatelet and anticoagulant drugs.
Based on these findings, nattokinase and similar products such as serrapeptase should undergo well-funded, accelerated preclinical and clinical development programs. The issue at hand is the urgency of time, similar to that with SARS-CoV-2 infection and empiric early therapy. It will take up to 20 years to have a fully developed pharmaceutical profile to characterize the safety and efficacy of nattokinase in the treatment of vaccine injury and post-COVID syndromes. Large number of people are sick now and many believe empiric treatment is justified given sufficiently low risk of side effects and potentially high reward. My recommendation is to discuss this with your doctor or seek a specialist in holistic or naturopathic medicine who is experienced with the safety profile of nattokinase in a range of applications.
If you find “Courageous Discourse” enjoyable and useful to your endeavors, please subscribe as a paying or founder member to support our efforts in helping you engage in these discussions with family, friends, and your extended circles.
Source:Courageous Discourse™ with Dr. Peter McCullough & John Leake is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Dr. Peter McCullough joins Alex Jones live in studio to give his powerful presentation on the COVID virus, its mutations, and the mRNA gene therapy/viral vector injections.
Segment 1 – Introduction
In this segment Dr. Peter McCullough touches on the public policy decisions in response to Covid-19 that have resulted in mass death, and the current international lawsuits alleging intentional crimes against humanity. The Doctor goes onto provide a big picture analysis of C19’s origins at the Wuhan Lab, and distinctions between it’s variants. This segment provides the basis for the detailed presentations that follow including: facts about the viral lifecycle, Euler’s Ratchet, the importance of early treatment, Omicron vs Delta, confirmation that no test currently exists to identify variant identity, and finally citations from the study conducted on American loss of life due to the vaccines.
Segment 2 – The Great Gamble of C19 Vaccine Development
In the second part of Dr. McCullough’s InfoWars interview contrary to CDC/NIH guidelines the Doctor extols the urgent need for early ambulatory therapy for successful Covid-19 treatment. Dr. McCullough prefaces the discussion of experimental mRNA and adenovirus injections with review of an article titled, “The Great Gamble of C19 Vaccine Development.” This sets the stage for a deep dive into the origins of the C19 Spike Protein, and its mechanism of action. The segment culminates in corroboration of the Whuhan Lab theory, and a detailed explanation how vaccine damage occurs, and the tissues affected.
Segment 3- Medical Censorship & Countervailing Evidence
Dr. McCullough describes the attacks being waged on members of the medical community who publish examinations of the empirical evidence demonstrating Covid-19 vaccine damage. This includes an analysis of VAERS data showing disproportionate instances of myocarditis among men of all ages, plus a study using census data revealing up to 180,000 American deaths linked to the vaccine, making it a bigger killer than the illness. Finally, Dr. McCullough exposes the Regulatory Malfeasance occurring as CNN diabolically attempts to seduce young children to take the deadly vaccines through promotions running on Sesame Street.
A current lawsuit is challenging the secrecy of Pfizer’s vaccine trial data. Dr. Peter McCullough is one of the lead experts tasked with reviewing the data should the suit prevail. Currently, the fact pattern demonstrates zero transparency between the US Government and Pfizer. What are they hiding? The first priority is to “Do no harm” and safety is valued higher than efficacy, but Pfizer is attempting to seal all trial data for 70 years making product safety evaluations nearly impossible, while the Government is failing to conduct reviews according to statutory and historical measures. Dr. Peter McCullough advises the audience on the best way to stay healthy.
Dr. McCullough examines a recent study involving 780,000 VA Veterans. This and 22 other studies show waning vaccine efficacy over 3-6 months for all vaccines against all variants. Statistically this evidence demonstrates just a 1% mortality benefit, without addressing adverse events in adults, and young people geting no medical benefits from Covid-19 vaccination. With the waning efficacy, what does this mean going forward? Dr. Peter McCullough and Alex Jones predict increasing vaccine frequency tied to travel, work, etc. With Pfizer knowing about 1000’s of deaths following vaccination, is this part of a depopulation agenda?
The segment begins in review of the timeline and development of the Covid-19 pandemic including the well documented simulations preceding the outbreak that lead many to believe we are experiencing a well planned and orchestrated crisis.
Dr. McCullough reveals the genomic sequencing of the Omicron variant, which is unique from all previous strains of Covid. Omicron differs across 26 mutations occurring at the Receptor Binding Domain for ACE2 receptor sites, making this variant much less invasive than its predecessors. Dr. McCullough notes the presence of insertions in the Omicron genetic code, which are distinct from mutations, and could possibly indicate evidence of engineering.
Dr. McCullough also dispels the false claim that Omicron should be blamed on the unvaccinated, citing a study from Denmark showing 79% of Omicron infections occurring in fully vaccinated patients.
Alex Jones and Dr. McCullough discuss the war being waged against honest medical professionals attempting to save lives by revealing disastrous public policy measures in response to Covid-19. Examples include forced vaccination policies within hospitals like Houston Methodist, that have aggressively coerced staff to take the vaccination or face termination of employment. The result is these institutions are now facing shortages due to attrition of staff that resist such measures, and loss of staff due to high infection rates despite nearly 100% vaccination. The Doctor also touches on reactivation diseases resulting from immunosuppression, durability of immunity, and a pattern of the Government blocking effective therapeutics in favor of deadly vaccines.
Topics include federal monoclonal rationing, and CDC exoneration of unvaccinated as causing the pandemic by their own statistics. Dr. McCullough breaks down effective Early Outpatient Treatment Protocol consisting of: 1) Precautionary principle – mass casualty event, 2) Comprehensive evidence signalling, 3) Acceptable safety, and 4) Drugs in combination. Gold standard randomized trials indicate viracidal treatments with Iodine, H2O2, Colloidal Silver, and 03 are highly effective in stopping viral replication within the nasal passage.
Top Scientists call on the World Health Organization to shut down vaccinations against Omicron. Dr. McCullough describes the case for crimes against humanity, and issues an optimistic message for humanity.
Sovereign’s Handbook by Johnny Liberty (30th Anniversary Edition) (3-Volume Printed, Bound Book or PDF)
A three-volume, 750+ page tome with an extensive update of the renowned underground classic ~ the Global Sovereign’s Handbook. Still after all these years, this is the most comprehensive book on sovereignty, economics, law, power structures and history ever written. Served as the primary research behind the best-selling Global One Audio Course. Available Now!
Dawning of the Corona Age: Navigating the Pandemic by Johnny Freedom (3rd Edition) (Printed, Bound Book or PDF)
This comprehensive book, goes far beyond the immediate impact of the “pandemic”, but, along with the reader, imagines how our human world may be altered, both positively and negatively, long into an uncertain future. Available Now!
OMNS (Oct. 18, 2021) No issue in the history of medicine has been as strident and polarized as that of the risk/benefit profiles of the various COVID vaccines being administered around the world. This article does not seek to clarify this issue to the satisfaction of either the pro-vaccine or the anti-vaccine advocates. However, all parties should realize that some toxicity does result in some vaccinated individuals some of the time, and that such toxicity can sometimes be unequivocally attributed to the preceding administration of the vaccine. Whether this toxicity occurs often enough and with great enough severity in vaccinated persons to be of greater concern than dealing with the contraction and evolution of COVID infections remains the question for many people.
Practically speaking, it does not matter whether an adverse event that occurs after a vaccination gets “blamed” on the vaccination. Such a matter may never get resolved. The issue of greatest concern is whether that adverse event can be clinically resolved if not effectively prevented, and whether any long-term damage to the body can be prevented once an adverse event is recognized. The remainder of this article will address the etiologies of such damage along with measures that can mitigate or even resolve such damage.
Toxins and Oxidative Stress
All toxins ultimately inflict their damage by directly oxidizing biomolecules, or by indirectly resulting in the oxidation of those biomolecules (proteins, sugars, fats, enzymes, etc.). When biomolecules becomes oxidized (lose electrons) they can no longer perform their normal chemical or metabolic functions. No toxin can cause any clinical toxicity unless biomolecules end up becoming oxidized. The unique array of biomolecules that become oxidized determines the nature of the clinical condition resulting from a given toxin exposure. There is no “disease” present in a cell involved in a given medical condition beyond the distribution and degree of biomolecules that are oxidized. Rather than “causing” disease, the state of oxidation in a grouping of biomolecules IS the disease.
When antioxidants can donate electrons back to oxidized biomolecules (reduction), the normal function of these biomolecules is restored (Levy, 2019). This is the reason why sufficient antioxidant therapy, such as can be achieved by highly-dosed intravenous vitamin C, has proven to be so profoundly effective in blocking and even reversing the negative clinical impact of any toxin or poison. There exists no toxin against which vitamin C has been tested that has not been effectively neutralized (Levy, 2002). There is no better way to save a patient clinically poisoned by any agent than by immediately administering a sizeable intravenous infusion of sodium ascorbate. The addition of magnesium chloride to the infusion is also important to protect against sudden life-threatening arrhythmias that can occur before a sufficient number of the newly-oxidized biomolecules can be reduced and any remaining toxin is neutralized and excreted.
Abnormal Blood Clotting
Both the COVID vaccine and the COVID infection have been documented to provoke increased blood clotting [thrombosis] (Biswas et al., 2021; Lundstrom et al., 2021). Viral infections in general have been found to cause coagulopathies resulting in abnormal blood clotting (Subramaniam and Scharrer, 2018). Critically ill COVID ICU patients demonstrated elevated D-dimer levels roughly 60% of the time (Iba et al., 2020). An elevated D-dimer test result is almost an absolute confirmation of abnormal blood clotting taking place somewhere in the body. Such clots can be microscopic, at the capillary level, or much larger, even involving the thrombosis of large blood vessels. Higher D-dimer levels that persist in COVID patients appear to directly correlate with significantly increased morbidity and mortality (Naymagon et al., 2020; Paliogiannis et al., 2020; Rostami and Mansouritorghabeh, 2020).
Platelets, the elements of the blood that can get sticky and both initiate and help grow the size of blood clots, will generally demonstrate declining levels in the blood at the same time D-dimer levels are increasing, since their stores are being actively depleted. A post-vaccination syndrome known as vaccine-induced prothrombotic immune thrombocytopenia (VIPIT) with these very findings has been described (Favaloro, 2021; Iba et al., 2021; Scully et al., 2021; Thaler et al., 2021). Vaccinations have also been documented to cause bleeding syndromes due to autoimmune reactions resulting in low platelet levels (Perricone et al., 2014).
This can create some confusion clinically, as chronically low platelet levels by themselves can promote clinical syndromes of increased bleeding rather than increased blood clotting. As such, some primary low platelet disorders require pro-coagulation measures to stop bleeding, while other conditions featuring primary increased thrombosis with the secondary rapid consumption of platelet stores end up needing anticoagulation measures to stop that continued consumption of platelets (Perry et al., 2021). Significant thrombosis post-vaccination in the absence of an elevated D-dimer level or low platelet count has also been described (Carli et al., 2021). In platelets taken from COVID patients, platelet stickiness predisposing to thrombosis has been shown to result from spike protein binding to ACE2 receptors on the platelets (Zhang et al., 2021).
Of note, a D-dimer test that is elevated due to increased blood clotting will usually only stay elevated for a few days after the underlying pathology provoking the blood clotting has been resolved. Chronic, or “long-haul” COVID infections, often demonstrate persistent evidence of blood clotting pathology. In one study, 25% of convalescent COVID patients who were four months past their acute COVID infections demonstrated increased D-dimer levels. Interestingly, these D-dimer elevations were often present when the other common laboratory parameters of abnormal blood clotting had returned to normal. These other tests included prothrombin time, partial thromboplastin time, fibrinogen level, and platelet count. Inflammation parameters, including C-reactive protein and interleukin-6, typically also had returned to normal (Townsend et al., 2021).
Persistent evidence of blood clotting (increased D-dimer levels) in chronic COVID patients might be a reliable way to determine the persistent presence/production of the COVID spike protein. Another way, discussed below, might be dark field microscopy to look for rouleaux formation of the red blood cells (RBCs). At the time of the writing of this article, the correlation between an increased D-dimer level and rouleaux formation of the RBCs remains to be determined. Certainly, the presence of both should trigger the greatest of concern for the development of significant chronic COVID and post-COVID vaccination complications.
Is Persistent Spike Protein the Culprit?
Spike proteins are the spear-like appendages attached to and completely surrounding the central core of the COVID virus, giving the virion somewhat of a porcupine-like appearance. Upon binding to the angiotensin converting enzyme 2 (ACE2) receptors on the cell membranes of the target cells, dissolving enzymes are released that then permit entry of the complete COVID virus into the cytoplasm, where replication of the virus can ensue (Belouzard et al., 2012; Shang et al., 2020).
Concern has been raised regarding the dissemination of the spike protein throughout the body after vaccination. Rather than staying localized at the injection site in order to provoke the immune response and nothing more, spike protein presence has been detected throughout the body of some vaccinated individuals. Furthermore, it appears that some of the circulating spike proteins simply bind the ACE2 receptors without entering the cell, inducing an autoimmune response to the entire cell-spike protein entity. Depending on the cell type that binds the spike protein, any of a number of autoimmune medical conditions can result.
While the underlying pathology remains to be completely defined, one explanation for the problems with thrombotic tendencies and other symptomatology seen with chronic COVID and post-vaccination patients relates directly to the persistent presence of the spike protein part of the coronavirus. Some reports assert that the spike protein can continue to be produced after the initial binding to the ACE2 receptors and entry into some of the cells that it initially targets. The clinical pictures of chronic COVID and post-vaccine toxicity appear very similar, and both are likely due to this continued presence, and body-wide dissemination, of the spike protein (Mendelson et al., 2020; Aucott and Rebman, 2021; Levy, 2021; Raveendran, 2021).
Although they are found on many different types of cells throughout the body, the ACE2 receptors on the epithelial cells lining the airways are the first targets of the COVID virus upon initial encounter when inhaled (Hoffman et al., 2020). Furthermore, the concentration of these receptors is especially high on lung alveolar epithelial cells, further causing the lung tissue to be disproportionately targeted by the virus (Alifano et al., 2020). Unchecked, this avid receptor binding and subsequent viral replication inside the lung cells leads directly to low blood oxygen levels and the adult respiratory distress syndrome [ARDS] (Batah and Fabro, 2021). Eventually there is a surge of intracellular oxidation known as the cytokine storm, and death from respiratory failure results (Perrotta et al., 2020; Saponaro et al., 2020; Hu et al., 2021).
COVID, Vaccination, and Oxidative Stress
Although some people have prompt and clear-cut negative side effects after COVID vaccination, many appear to do well and feel completely fine after their vaccinations. Is this an assurance that no harm was done, or will be done, by the vaccine in such individuals? Some striking anecdotal evidence suggests otherwise, while also indicating that there exist good options for optimal protection against side effects in both the short- and long-term.
Under conditions of inflammation and systemically increased oxidative stress, RBCs can aggregate to varying degrees, sometimes sticking together like stacks of coins with branching of the stacks seen when the stickiness is maximal. This is known as rouleaux formation of the RBCs (Samsel and Perelson, 1984). When this rouleaux formation is pronounced, increased blood viscosity (thickness) is seen, and there is increased resistance to the normal, unimpeded flow of blood, especially in the microcirculation (Sevick and Jain, 1989; Kesmarky et al., 2008; Barshtein et al., 2020; Sloop et al., 2020).
With regard to the smallest capillaries through which the blood must pass, it needs to be noted that individual RBCs literally need to fold slightly to pass from the arterial to the venous side, as the capillary diameter at its narrowest point is actually less than the diameter of a normal RBC, or erythrocyte. It is clear that any aggregation of the RBCs, as is seen with rouleaux formation, will increase resistance to normal blood flow, and it will be more pronounced as the caliber of the blood vessel decreases. Not surprisingly, rouleaux formation of the RBCs is also associated with an impaired ability of the blood to optimally transport oxygen, which notably is another feature of COVID spike protein impact (Cicco and Pirrelli, 1999). Increased RBC aggregation has been observed in a number of different microcirculatory disorders, and it appears to be linked to the pathophysiology in these disorders.
Rouleaux formation is easily visualized directly with dark field microscopy. When available, feedback is immediate, and there is no need to wait for a laboratory to process a test specimen. It is a reliable indicator of abnormal RBC stickiness and increased blood viscosity, typically elevating the erythrocyte sedimentation test (ESR), an acute phase reactant test that consistently elevates along with C-reactive protein in a setting of generalized increased oxidative stress throughout the body (Lewi and Clarke, 1954; Ramsay and Lerman, 2015). As such, it can never be dismissed as an incidental and insignificant finding, especially in the setting of a symptom-free individual post-vaccination appearing to be normal and presumably free of body-wide increased inflammation and oxidative stress. States of advanced degrees of increased systemic oxidative stress, as is often seen in cancer patients, can also display rouleaux formation among circulating neoplastic cells and not just the RBCs (Cho, 2011).
Rouleaux Formation Post-COVID Vaccination
The dark field blood examinations seen below come from a 62-year-old female who had received the COVID vaccination roughly 60 days earlier. The first picture reveals mild rouleaux formation of the blood. After a sequence of six autohemotherapy ozone passes, the second picture shows a completely normal appearance of the RBCs.
A second patient, a young adult male who received his vaccination 15 days earlier without any side effects noted and feeling completely well at the time, had the dark field examination of his blood performed. This first examination seen below revealed severe rouleaux formations of the RBCs with extensive branching, appearing to literally involve all of the RBCs visualized in an extensive review of multiple different microscopic fields. He then received one 400 ml ozonated saline infusion followed by a 15,000 mg infusion of vitamin C. The second picture reveals a complete and immediate resolution of the rouleaux formation seen on the first examination. Furthermore, the normal appearance of the RBCs was still seen 15 days later, giving some reassurance that the therapeutic infusions had some durability, and possibly permanency, in their positive impact.
A third adult who received the vaccination 30 days earlier also had severe rouleaux formation on her dark field examination, and this was also completely resolved after the ozonated saline infusion followed by the vitamin C infusion. Of note, similar abnormal dark field microscopy findings were found in other individuals following Pfizer, Moderna, or Johnson & Johnson COVID vaccinations.
Preventing and Treating Chronic COVID and COVID Vaccine Complications
In addition to the mechanisms already discussed by which the spike protein can inflict damage, it appears the spike protein itself is significantly toxic. Such intrinsic toxicity (ability to cause the oxidation of biomolecules) combined with the apparent ability of the spike protein to replicate itself like a complete virus greatly increases the amount of toxic damage that can potentially be inflicted. A potent toxin is bad enough, but one that can replicate and increase its quantity inside the body after the initial encounter represents a unique challenge among toxins. And if the mechanism of replication can be sustained indefinitely, the long-term challenge to staying healthy can eventually become insurmountable. Nevertheless, this toxicity also allows it to be effectively targeted by high enough doses of the ultimate antitoxin, vitamin C, as discussed above. And even the continued production of spike protein can be neutralized by a daily multi-gram dosing of vitamin C, which is an excellent way to support optimal long-term health, anyway.
As was noted in an earlier article (Levy, 2021), there appear to be multiple ways to deal with spike protein effectively. The approaches to preventing and treating chronic COVID and COVID vaccine complications are similar, except that it would appear that a completely normal D-dimer blood test combined with a completely normal dark field examination of the blood could give the reassurance that the therapeutic goal has been achieved.
Until more data is accumulated on these approaches, it is probably advisable, if possible, to periodically reconfirm the normalcy of both the D-dimer blood test and the dark field blood examination to help assure that no new spike protein synthesis has resumed. This is particularly important since some patients who are clinically normal and symptom-free following COVID infection have been found to have the COVID virus persist in the fecal matter for an extended period of time (Chen et al., 2020; Patel et al., 2020; Zuo et al., 2020). Any significant immune challenge or new pathogen exposure facilitating a renewed surge of COVID virus replication could result in a return of COVID symptoms in such persons if the virus cannot be completely eliminated from the body.
Suggested Protocol (to be coordinated with the guidance of your chosen health care provider):
For individuals who are post-vaccination or symptomatic with chronic COVID, vitamin C should be optimally dosed, and it should be kept at a high but lesser dose daily indefinitely.
Ideally, an initial intravenous administration of 25 to 75 grams of vitamin C should be given depending on body size. Although one infusion would likely resolve the symptoms and abnormal blood examination, several more infusions can be given if feasible over the next few days.
An option that would likely prove to be sufficient and would be much more readily available to larger numbers of patients would be one or more rounds of vitamin C given as a 7.5 gram IV push over roughly 10 minutes, avoiding the need for a complete intravenous infusion setup, a prolonged time in a clinic, and substantially greater expense (Riordan-Clinic-IVC-Push-Protocol, 10.16.14.pdf).
Additionally, or alternatively if IV is not available, 5 grams of liposome-encapsulated vitamin C (LivOn Labs) can be given daily for at least a week.
When none of the above three options are readily available, a comparable positive clinical impact will be seen with the proper supplementation of regular forms of oral vitamin C as sodium ascorbate or ascorbic acid. Either of these can be taken daily in three divided doses approaching bowel tolerance after the individual determines their own unique needs (additional information, see Levy, vitamin C Guide in References; Cathcart, 1981).
An excellent way to support any or all of the above measures for improving vitamin C levels in the body is now available and very beneficial clinically. A supplemental polyphenol that appears to help many to overcome the epigenetic defect preventing the internal synthesis of vitamin C in the liver can be taken once daily. This supplement also appears to provide the individual with the ability to produce and release even greater amounts of vitamin C directly into the blood in the face of infection and other sources of oxidative stress (www.formula216.com).
Hydrogen peroxide (HP) nebulization (Levy, 2021, free eBook) is an antiviral and synergistic partner with vitamin C, and it is especially important in dealing with acute or chronic COVID, or with post-COVID vaccination issues. As noted above, the COVID virus can persist in the stool. In such cases, a chronic pathogen colonization (CPC) of COVID in the throat continually supplying virus that is swallowed into the gut is likely present as well, even when the patient seems to be clinically normal. This will commonly be the case when specific viral eradication measures were not taken during the clinical course of the COVID infection. HP nebulization will clear out this CPC, which will stop the continued seeding of the COVID virus in the gut and stool as well. Different nebulization approaches are discussed in the eBook.
When available, ozonated saline and/or ozone autohemotherapy infusions are excellent. Conceivably, this approach alone might suffice to knock out the spike protein presence, but the vitamin C and HP nebulization approaches will also improve and maintain health in general. Ultraviolet blood irradiation and hyperbaric oxygen therapy will likely achieve the same therapeutic effect if available.
Ivermectin, hydroxychloroquine, and chloroquine are especially important in preventing new binding of the spike protein to the ACE2 receptors that need to be bound in order for either the spike protein alone or for the entire virus to gain entry into the target cells (Lehrer and Rheinstein, 2020; Wang et al., 2020; Eweas et al., 2021). These agents also appear to have the ability to directly bind up any circulating spike protein before it binds any ACE2 receptors (Fantini et al., 2020; Sehailia and Chemat, 2020; Saha and Raihan, 2021). When the ACE2 receptors are already bound, the COVID virus cannot enter the cell (Pillay, 2020). These three agents also serve as ionophores that promote intracellular accumulation of zinc that is needed to kill/inactivate any intact virus particles that might still be present.
Many other positive nutrients, vitamins, and minerals are supportive of defeating the spike protein, but they should not be used to the exclusion of the above, especially the combination of highly-dosed vitamin C and HP nebulization.
Summary
As the pandemic continues, there is an increasing number of chronic COVID patients and patients post-COVID vaccination with a number of different symptoms. Furthermore, there is increasing number of vaccinated individuals who still end up contracting a COVID infection. This is resulting in a substantial amount of morbidity and mortality around the world. The presence and persistence of the COVID spike protein, along with the chronic colonization of the COVID virus itself in the aerodigestive tract as well as in the lower gut, appear to be major reasons for illness in this group of patients.
Persistent elevation of D-dimer protein in the blood and the presence of rouleaux formation of the RBCs, especially when advanced in degree, appear to be reliable markers of persistent spike protein-related illness. The measures noted above, particular the vitamin C and HP nebulization, should result in the disappearance of the D-dimer in the blood while normalizing the appearance of the RBCs examined with dark field microscopy. Even though new research is taking place daily that may modify therapeutic recommendations, it appears that taking the measures to eliminate D-dimer from the blood and to maintain a consistently normal morphological appearance of the blood is a very practical and efficient way to curtail the ongoing morbidity and mortality secondary to the persistent spike protein presence seen in chronic COVID and in post-COVID vaccination patients.
There are many vaccinated individuals who feel well yet remain cautious about potential future side effects, and who really have no easy access to D-dimer testing or dark field examination of their blood. Such persons can follow a broad-spectrum supplementation regimen featuring vitamin C, magnesium chloride, vitamin D, zinc, and a good multivitamin/multimineral supplement free of iron, copper, and calcium. Periodic but regular HP nebulization should be included as well. This regimen will offer good spike protein protection while optimizing long-term health. Furthermore, such a long-term supplementation regimen is advisable regardless of how much of the protocol discussed above is followed.
(OMNS Contributing Editor Dr. Thomas E. Levy is board certified in internal medicine and cardiology. He is also an attorney, admitted to the bar in Colorado and in the District of Columbia. The views presented in this article are the author’s and not necessarily those of all members of the Orthomolecular Medicine News Service Editorial Review Board.)
Ozone treatment is also supported by other research groups and papers:
Alifano M, Alifano P, Forgez P, Iannelli A (2020) Renin-angiotensin system at the heart of the COVID-19 pandemic. Biochemie 174:30-33. PMID: 32305506
Aucott J, Rebman A (2021) Long-haul COVID: heed the lessons from other infection-triggered illnesses. Lancet 397:967-968. PMID: 33684352
Barshtein G, Waynblum D, Yedgar S (2020) Kinetics of linear rouleaux formation studied by visual monitoring of red cell dynamic organization. Biophysical Journal 78:2470-2474. PMID: 10777743
Batah S, Fabro A (2021) Pulmonary pathology of ARDS in COVID-19: a pathological review for clinicians. Respiratory Medicine 176:106239. PMID: 33246294
Belouzard S, Millet J, Licitra B, Whittaker G (2012) Mechanisms of coronavirus cell entry mediated by the viral spike protein. Viruses 4:1011-1033. PMID: 22816037
Biswas S, Thakur V, Kaur P et al. (2021) Blood clots in COVID-19 patients: simplifying the curious mystery. Medical Hypotheses 146:110371. PMID: 33223324
Carli G, Nichele I, Ruggeri M, Barra S, Tosetto A (2021) Deep vein thrombosis (DVT) occurring shortly after the second dose of mRNA SARS-CoV-2 vaccine. Internal and Emergency Medicine 16:803-804. PMID: 336876791
Cathcart R (1981) Vitamin C, titrating to bowel tolerance, anascorbemia, and acute induced scurvy. Medical Hypotheses 7:1359-1376. PMID: 7321921
Chen Y, Chen L, Deng Q et al. (2020) The presence of SARS-CoV-2 RNA I the feces of COVID-19 patients. Journal of Medical Virology 92:833-840. PMID: 32243607
Cho S (2011) Plasma cell leukemia with rouleaux formation involving neoplastic cells and RBC. The Korean Journal of Hematology 46:152. PMID: 22065968
Cicci G, Pirrelli A (1999) Red blood cell (RBC) deformability, RBC aggregability and tissue oxygenation in hypertension. Clinical Hemorheology and Microcirculation 21:169-177. PMID: 10711739
Eweas A, Alhossary A, Abdel-Moneim A (2021) Molecular docking reveals ivermectin and remdesivir as potential repurposed drugs against SARS-CoV-2. Frontiers in Microbiology 11:592908. PMID: 33746908
Fantini J, Di Scala C, Chahinian H, Yahi N (2020) Structural and molecular modelling studies reveal a new mechanism of action of chloroquine and hydroxychloroquine against SARS-CoV-2 infection. International Journal of Antimicrobial Agents 55:105960. PMID: 32251731
Favaloro E (2021) Laboratory testing for suspected COVID-19 vaccine-induced (immune) thrombotic thrombocytopenia. International Journal of Laboratory Hematology 43:559-570. PMID: 34138513
Hoffman M, Kleine-Weber H, Schroeder S et al. (2020) SARS-CoV-2 entry depends on ACE 2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 181:271-280. PMID: 32142651
Hu B, Huang S, Yin L (2021) The cytokine storm and COVID-19. Journal of Medical Virology 93:250-256. PMID: 32592501
Iba T, Levy J, Levi M et al. (2020) Coagulopathy of coronavirus disease 2019. Critical Care Medicine 48:1358-1364. PMID: 32467443
Iba T, Levy J, Warkentin T (2021) Recognizing vaccine-induced immune thrombotic thrombocytopenia. Critical Care Medicine [Online ahead of print]. PMID: 34259661
Kesmarky G, Kenyeres P, Rabai M, Toth K (2008) Plasma viscosity: a forgotten variable. Clinical Hemorheology and Microcirculation 39:243-246. PMID: 18503132
Lehrer S, Rheinstein P (2020) Ivermectin docks to the SARS-CoV-2 spike receptor-binding domain attached to ACE 2. In Vivo 34:3023-3026. PMID: 32871846
Levy T (2021) Rapid Virus Recovery: No need to live in fear! Henderson, NV: MedFox Publishing. Free eBook download (English or Spanish) available at https://rvr.medfoxpub.com/
Lewi S, Clarke K (1954) Rouleaux formation intensity and E.S.R. British Medical Journal 2:336-338. PMID: 13182211
Lundstrom K, Barh D, Uhal B et al. (2021) COVID-19 vaccines and thrombosis-roadblock or dead-end street? Biomolecules 11:1020. PMID: 34356644
Mendelson M, Nel J, Blumberg L et al. (2020) Long-COVID: an evolving problem with an extensive impact. South African Medical Journal 111:10-12. PMID: 33403997
Naymagon L, Zubizarreta N, Feld J et al. (2020) Admission D-dimer levels, D-dimer trends, and outcomes in COVID-19. Thrombosis Research 196:99-105. PMID: 32853982
Paliogiannis P, Mangoni A, Dettori P et al. (2020) D-dimer concentrations and COVID-19 severity: a systematic review and meta-analysis. Frontiers in Public Health 8:432. PMID: 32903841
Patel K, Patel P, Vunnam R et al. (2020) Gastrointestinal, hepatobiliary, and pancreatic manifestations of COVID-19. Journal of Clinical Virology 128:104386. PMID: 32388469
Perricone C, Ceccarelli F, Nesher G et al. (2014) Immune thrombocytopenic purpura (ITP) associated with vaccinations: a review of reported cases. Immunologic Research 60:226-235. PMID: 25427992
Perrotta F, Matera M, Cazzola M, Bianco A (2020) Severe respiratory SARS-CoV2 infection: does ACE2 receptor matter? Respiratory Medicine 168:105996. PMID: 32364961
Perry R, Tamborska A, Singh B et al. (2021) Cerebral venous thrombosis after vaccination against COVID-19 in the UK: a multicentre cohort study. Lancet Aug 6. Online ahead of print. PMID: 34370972
Pillay T (2020) Gene of the month: the 2019-nCoV/SARS-CoV-2 novel coronavirus spike protein. Journal of Clinical Pathology 73:366-369. PMID: 32376714
Ramsay E, Lerman M (2015) How to use the erythrocyte sedimentation rate in paediatrics. Archives of Disease in Childhood. Education and Practice Edition 100:30-36. PMID: 25205237
Raveendran A (2021) Long COVID-19: Challenges in the diagnosis and proposed diagnostic criteria. Diabetes & Metabolic Syndrome: Clinical Research & Reviews 15:145-146. PMID: 33341598
Rostami M, Mansouritorghabeh H (2020) D-dimer level in COVID-19 infection: a systematic review. Expert Review of Hematology 13:1265-1275. PMID: 32997543
Saha J, Raihan M (2021) The binding mechanism of ivermectin and levosalbutamol with spike protein of SARS-CoV-2. Structural Chemistry Apr 12. Online ahead of print. PMID: 33867777
Samsel R, Perelson A (1984) Kinetics of rouleau formation. II. Reversible reactions. Biophysical Journal 45:805-824. PMID: 6426540
Saponaro F, Rutigliano G, Sestito S et al. (2020) ACE 2 in the era of SARS-CoV-2: controversies and novel perspectives. Frontiers in Molecular Biosciences 7:588618. PMID: 33195436
Scully M, Singh D, Lown R et al. (2021) Pathologic antibodies to platelet factor 4 after ChAdOx1 nCoV-19 vaccination. The New England Journal of Medicine 384:2202-2211. PMID: 33861525
Sehailia M, Chemat S (2021) Antimalarial-agent artemisinin and derivatives portray more potent binding of Lys353 and Lys31-binding hotspots of SARS-CoV-2 spike protein than hydroxychloroquine: potential repurposing of artenimol for COVID-19. Journal of Biomolecular Structure & Dynamics 39:6184-6194. PMID: 32696720
Sevick E, Jain R (1989) Viscous resistance to blood flow in solid tumors: effect of hemocrit on intratumor blood viscosity. Cancer Research 49:3513-3519. PMID: 2731173
Shang J, Wan Y, Luo C et al. (2020) Cell entry mechanisms of SARS-CoV-2. Proceedings of the National Academy of Sciences of the United States of America 117:11727-11734. PMID: 32376634
Sloop G, De Mast Q, Pop G et al. (2020) The role of blood viscosity in infectious diseases. Cureus 12:e7090. PMID: 32226691
Subramaniam S, Scharrer I (2018) Procoagulant activity during viral infections. Frontiers in Bioscience 23:1060-1081. PMID: 28930589
Thaler J, Ay C, Gleixner K et al. (2021) Successful treatment of vaccine-induced prothrombotic immune thrombocytopenia (VIPIT). Journal of Thrombosis and Haemostasis 19:1819-1822. PMID: 33877735
Townsend L, Fogarty H, Dyer A et al. (2021) Prolonged elevation of D-dimer levels in convalescent COVID-19 patients is independent of the acute phase response. Journal of Thrombosis and Haemostasis 19:1064-1070. PMID: 33587810
Wang N, Han S, Liu R et al. (2020) Chloroquine and hydroxychloroquine as ACE2 blockers to inhibit viropexis of 2019-nCoV spike pseudotyped virus. Phytomedicine: International Journal of Phytotherapy and Phytopharmacology 79:153333. PMID: 32920291
Zhang S, Liu Y, Want X et al. (2021) SARS-Cov-2 binds platelet ACE2 to enhance thrombosis in COVID-19. Journal of Hematology & Oncology 13:120. PMID: 32887634
Zuo T, Zhang F, Lui G et al. (2020) Alterations in gut microbiota of patients with COVID-19 during time of hospitalization. Gastroenterology 159:944-955. PMID: 32442562
Sovereign’s Handbook by Johnny Liberty (30th Anniversary Edition) (3-Volume Printed, Bound Book or PDF)
A three-volume, 750+ page tome with an extensive update of the renowned underground classic ~ the Global Sovereign’s Handbook. Still after all these years, this is the most comprehensive book on sovereignty, economics, law, power structures and history ever written. Served as the primary research behind the best-selling Global One Audio Course. Available Now!
Dawning of the Corona Age: Navigating the Pandemic by Johnny Freedom (3rd Edition) (Printed, Bound Book or PDF)
This comprehensive book, goes far beyond the immediate impact of the “pandemic”, but, along with the reader, imagines how our human world may be altered, both positively and negatively, long into an uncertain future. Available Now!
I’m a practicing ER nurse of 25 years. The amount of blood clots, strokes, cardiac events like myocarditis/pericarditis, Bell’s Palsy, shingles, etc. that I’ve seen since the vaccine rollout is more than I’ve ever seen in the previous 23.5 years combined.
I don’t know how anyone can’t be frightened by what we are seeing. When I try to discuss this with my coworkers, they turn their heads and look downcast, but will rarely speak.
I think it’s because like me, they feel betrayed for following the narrative, but unlike me they won’t open their eyes and speak out (they’re afraid for their careers and also are scared to death that their bodies are ticking time bombs). It’s easier to ignore than to acknowledge. – Susan Pace, Medscape
The fact that there is a crisis in the U.S. medical system is not in dispute, as even the corporate media has been covering this since 2021, as many hospital Emergency Rooms across the U.S. have either closed down completely, or reduced their hours, due to lack of staffing.
One of the most recent closings happened at Wellstar’s Atlanta Medical Center in Southwest Atlanta, a predominantly Black community. (Source.)
Earlier this month (November 2022) a group of medical organizations that include the American Medical Association and American Psychiatric Association warned President Biden that hospital emergency departments were reaching a “breaking point” as they deal with influxes of patients seeking beds that are not available.
“Our nation’s safety net is on the verge of breaking beyond repair; EDs are gridlocked and overwhelmed with patients waiting — waiting to be seen; waiting for admission to an inpatient bed in the hospital; waiting to be transferred to psychiatric, skilled nursing, or other specialized facilities; or, waiting simply to return to their nursing home,” the groups said in their letter to Biden. (Source.)
A report from commercial intelligence company Definitive Healthcare earlier this month stated that 334,000 physicians, nurse practitioners, physician assistants and other clinicians left the workforce in 2021.
Physicians experienced the largest loss, with 117,000 professionals leaving the workforce in 2021, followed by nurse practitioners, with 53,295 departures, and physician assistants, with 22,704 departures. About 22,000 physical therapists also left the healthcare workforce and 15,500 licensed clinical social workers, according to a report from commercial intelligence company Definitive Healthcare.
Among physician specialties, the biggest declines were seen within internal medicine, family practice and emergency medicine fields. “Like clinicians and registered nurses, providers in these three specialties frequently worked on the frontlines during the pandemic, risking exposure and facing many of the same pressures and stressors as described earlier,” the report authors wrote.
In 2021, 15,000 internal medicine doctors left the workforce, followed by 13,015 providers who left family practice and 10,874 who left clinical psychology.
Definitive Healthcare’s report leverages data from more than 2 million physicians and nurses, 9,200 hospitals and IDNs and 128,000 physician groups. (Source.)
While statistics for 2022 are not available yet as the year has not yet finished, a survey conducted back in March this year revealed that one third of the nation’s nurses were planning on leaving their jobs in 2022. (Source.)
Becker Hospital Review reported today that cash reserves, an important indicator of financial stability, are dropping for hospitals and health systems across the U.S. (Source.) Fewer staff to treat patients equals less customers which leads to lost revenue.
These are facts that nobody is disputing.
However, when we look at the reasons why these medical staff have left their jobs, there appear to be certain reasons that are not allowed to be mentioned or discussed in the corporate news media. The usual reasons that corporate news media give, which are heavily funded by Big Pharma, are: “retirement, burnout and pandemic-related stressors.”
What is never addressed, however, is how many of these medical professionals, most of whom were mandated to take the experimental COVID-19 vaccines, have died or were disabled following the COVID-19 shots.
As we have previously reported, sources in Canada have already found over 80 doctors who have died following the COVID-19 shots. See:
The other reason that is never reported in the corporate news, is the emotional and mental state of medical professionals who still work in the system, and who have come to realize what these deadly shots actually do, but are too afraid to speak out.
Fortunately, some have dared to speak out, such as nurse Susan Pace who I quoted at the beginning of this article from a forum for medical professionals on Medscape. This forum is a rare place on the Internet where medical professionals have spoken out on the injuries and deaths following the COVID-19 shots, as medical professionals were among the first to be injected with these experimental “vaccines,” and many have gone there to look for help in overcoming their injuries.
We covered many of their testimonies in June of last year:
The Conejo Guardian, an independent news organization in Ventura County, California, has also given a voice to some of these medial professionals who have spoken out regarding the injuries they have seen following COVID injections that we have republished:
Time to Leave the Corrupt Medical System
The medical system is collapsing, and there is no possible way to reform it or save it without dealing with the corruption in the system, starting with the criminal COVID-19 vaccines.
Most of those who know the truth about the COVID-19 vaccines and how deadly they are, have already left the system. Therefore, the ones that remain are mostly pro-vaccine, or not willing to sacrifice their careers to take a stand against the criminal corruption that unleashed the COVID-19 vaccines onto the public.
No wonder the nation’s hospitals and Emergency Rooms are overcrowded, or being forced to close. The reason is as plain as day, but the corporate media won’t report it.
And there are no political or judicial solutions to this problem, as both the Democrats and the Republicans are pro-vaccine, as is the U.S. Supreme Court. Big Pharma owns them.
You will not find relief there.
The only option left is to stop using the medical system. The system for the most part does not heal anyone anyway, as that is a terrible business model.
It is a very profitable “disease management” system, and the depth of corruption that exists within it has been completely exposed by the COVID-19 scam, as literally tens of thousands, if not hundreds of thousands, of doctors and medical professionals around the world successfully treated the symptoms of COVID-19 with a near 100% success rate using older drugs already in the market, as well as natural remedies.
The entire system is collapsing, so this is a good time to start learning how to take care of your own health without relying on the “experts” who have sold their souls to remain in a very evil business.
As the system collapses, new economic opportunities will arise for those who still have a soul and a conscience, to provide alternatives, especially in trauma care.
But it will be a huge fight, because the Globalists will not just stand by and allow this to happen. It will take a significant portion of the population to be willing to support new private businesses who separate themselves from government funding like Medicare and Medicaid. And once insurance companies wake up and admit that the most profitable people to insure are those who rejected the COVID vaccines, opportunities will arise to make private health services more affordable as well.
Sadly, very few will take this advice. Too many are still waiting for a savior, like Donald Trump or Ron DeSantis, to come in and fix everything.
It’s not going to happen. But if you haven’t figured that out by now, you probably never will. As you continue to use and trust in the medical system, your chances of dying in an over-crowded emergency room somewhere will continue to increase.
The Great Reset is coming, and those who know how to take care of their own health and not trust the evil and corrupt medical system, but instead put their trust in the One who can truly heal, will endure the hardships that are coming much better than those who do not.
Bless the LORD, O my soul, and forget not all his benefits, who forgives all your iniquity, who heals all your diseases, who redeems your life from the pit, who crowns you with steadfast love and mercy, who satisfies you with good so that your youth is renewed like the eagle’s. (Psalms 103:2-5)
Sovereign’s Handbook by Johnny Liberty (30th Anniversary Edition) (3-Volume Printed, Bound Book or PDF)
A three-volume, 750+ page tome with an extensive update of the renowned underground classic ~ the Global Sovereign’s Handbook. Still after all these years, this is the most comprehensive book on sovereignty, economics, law, power structures and history ever written. Served as the primary research behind the best-selling Global One Audio Course. Available Now!
Dawning of the Corona Age: Navigating the Pandemic by Johnny Freedom (3rd Edition) (Printed, Bound Book or PDF)
This comprehensive book, goes far beyond the immediate impact of the “pandemic”, but, along with the reader, imagines how our human world may be altered, both positively and negatively, long into an uncertain future. Available Now!
That’s a more radical decision than it might sound, but what he, and others, are finding is disturbing.
According to Sasha Latypova, a scientist with 25 years of experience in clinical trials for pharmaceutical companies, the contract between Pfizer and the US government prohibits independent researchers from studying the vaccines.
They claim it would ‘divert’ these precious resources away from their intended use fulfilling an ‘urgent’ need.
Is that true in Australia? Who knows? All the Commonwealth Department of Health has said about its contract with Pfizer is that it is commercial-in-confidence.
The Therapeutic Goods Administration performs tests on all Covid vaccines for composition and strength, purity and integrity, identity and endotoxins, but it provides scant details other than the batch numbers tested and whether they passed. (Spoiler alert: they did.)
In the US, the Centers for Disease Control specifically states that all Covid-19 vaccines are free from ‘metals, such as iron, nickel, cobalt, lithium, and rare earth alloys’ and ‘manufactured products such as micro-electronics, electrodes, carbon nanotubes, and nanowire semiconductors’.
Notably, this list does not include graphene oxide which has been widely investigated for biomedical applications. Some researchers sing its praises, its ‘ultra-high drug-loading efficiency due to the wide surface area’, its exceptional ‘chemical and mechanical constancy, sublime conductivity and excellent biocompatibility’.
But there’s a catch. ‘The toxic effect of graphene oxide on living cells and organs’ is ‘a limiting factor’ on its use in the medicine.
So is there graphene oxide in the Pfizer shots?
What Nixon found, and filmed, is bizarre to say the least. Inside a droplet of vaccine are strange mechanical structures.
They seem motionless at first but when Nixon used time-lapse photography to condense 48 hours of footage into two minutes, it showed what appear to be mechanical arms assembling and disassembling glowing rectangular structures that look like circuitry and micro chips.
These are not ‘manufactured products’ in the CDC’s words because they construct and deconstruct themselves but the formation of the crystals seems to be stimulated by electromagnetic radiation and stops when the slide with the vaccine is shielded by a Faraday bag.
Nixon’s findings are similar to those of teams in New Zealand, Germany, Spain and South Korea.
An Italian group led by Riccardo Benzi Cipelli analysed the blood of over 1,000 people, one month after they were vaccinated, who had been referred for tests because they had experienced side effects.
They ranged in age from 15 to 85 and had had between one and three doses. More than 94 per cent had abnormal readings, deformed red blood cells, reduced in counts and clumped around luminescent foreign objects which also attracted clusters of fibrin.
Some of the foreign objects dotted the blood like a starry night, some self-assembled into crystalline structures and others into spindly branches and tubes.
The Italians think the objects are metallic particles and say they resemble ‘graphene oxide and possibly other metallic compounds’.
They believe the damaged blood is contributing to post-vaccine coagulation disorders, which in turn contribute to increased malignancies, while graphene-family materials are associated with oxidative stress, DNA damage, inflammation and damage to those parts of the immune system that suppress tumours.
The artificial mRNA concoction which is ‘cloaked’ from the recipient’s immune system is also likely to reduce the recipients immune function, increasing the likelihood of new or recurring tumours.
Nixon has shared his findings with Wendy Hoy, professor of medicine at the University of Queensland who has called on the Australian government and its health authorities to explain the apparent spontaneous formation of chips and circuitry in mRNA vaccines when left at room temperature, and the abnormal objects that can be seen in the blood of vaccinated people.
Hoy thinks that these are ‘undoubtedly contributing to poor oxygen delivery to tissues and clotting events, including heart attacks and strokes’ and asks why there is no systematic autopsy investigation of deaths to investigate the role of the vaccine in Australia’s dramatic rise in mortality.
According to the latest data from the Australian Bureau of Statistics, excess mortality was over 17 percent in July. It is similarly elevated in other highly vaccinated populations.
In Germany, excess mortality in people over 60 increased by 174 percent between 20 September 2021, when 85 per cent of people over 60 were fully vaccinated, and October 2022.
In the UK, there have been more excess deaths in the last three months than at any time during the pandemic or indeed since 2010. In the most recent week, excess mortality in England was 16 percent.
In the US, excess mortality in people aged 25 to 44, and in those aged 75 to 84, is 18 per cent, and it is 15 percent in those aged 65 to 74.
The situation is all the more alarming because there should be fewer deaths now.
There has also been a dramatic rise in people with disabilities.
As for Covid, in Australia, vaccine efficacy appears to be negative, judging by the statistics in NSW which are far from perfect but the best in Australia.
They show that 88 per cent of people who died were vaccinated even though they made up only 85.5 per cent of the population. They also showed that the unvaccinated made up only 0.15 per cent of people in hospital with Covid and only 1.1 per cent of people in ICU.
Why is this? Almost certainly, because the unvaccinated who die of Covid in NSW are frail and elderly with multiple comorbidities, living in aged care or palliative care or at home, and don’t go to hospital.
Why weren’t they vaccinated? Probably because they or their doctors feared it would kill them.
The question is, how many others is it killing too?
Until health authorities tell us what’s in the shots, we won’t know.
Sovereign’s Handbook by Johnny Liberty (30th Anniversary Edition) (3-Volume Printed, Bound Book or PDF)
A three-volume, 750+ page tome with an extensive update of the renowned underground classic ~ the Global Sovereign’s Handbook. Still after all these years, this is the most comprehensive book on sovereignty, economics, law, power structures and history ever written. Served as the primary research behind the best-selling Global One Audio Course. Available Now!
Dawning of the Corona Age: Navigating the Pandemic by Johnny Freedom (3rd Edition) (Printed, Bound Book or PDF)
This comprehensive book, goes far beyond the immediate impact of the “pandemic”, but, along with the reader, imagines how our human world may be altered, both positively and negatively, long into an uncertain future. Available Now!
Syringes containing the Moderna Covid-19 vaccination for 6 month olds to 5 year olds lay on a table waiting to be used at Temple Beth Shalom in Needham, Massachusetts, on June 21, 2022.
The temple was one of the first sites in the state to offer vaccinations to anyone in the public. – US health authorities on June 18, 2022, cleared the Pfizer and Moderna Covid-19 vaccines for children aged five and younger, in a move President Joe Biden greeted as a “monumental step” in the fight against the virus. (Photo by Joseph Prezioso / AFP) (Photo by JOSEPH PREZIOSO/AFP via Getty Images)
By Zachary Stieber
Officials across the United States are continuing to spread misinformation about COVID-19 vaccines, The Epoch Times has found.
The claims include unsupported or misleading statements about vaccine effectiveness and safety.
The vast majority of officials responsible for the misinformation were unable or unwilling to provide evidence backing their claims.
The Louisiana Department of Health is among those exaggerating vaccine effectiveness. The agency claims in a promotional message that the vaccines “are 100% effective at preventing serious hospitalizations and deaths.”
The message does not cite any evidence and the department did not respond to a request for comment.
Clinical trials for the Moderna and Pfizer vaccines estimatedeffectiveness against severe illness at 100 percent, but studies since then have shown the protection starts much lower and drops quickly. That’s led to the clearance and recommendation of boosters, which confer a boost that also wanes.
Louisiana’s statement is one of many that rely on data from 2021, before the Omicron virus variant emerged, or even 2020. That data has little connection with the present state of the pandemic.
South Dakota’s health department, meanwhile, says that “Nearly everyone in the United States who is getting severely ill, needing hospitalization, and dying from COVID-19 is unvaccinated.”
Such statements are “directly related” to the drop in public confidence in health authorities during the pandemic, Dr. Jay Bhattacharya, a professor of medicine at Stanford University, told The Epoch Times after reviewing a sample of the claims.
“The public understands when they’re being manipulated,” he added.
Many state health agencies are offering falsehoods about COVID-19 vaccine safety and effectiveness, or downplaying negative information about the shots—a continuation of a trend that dates back to when the vaccines became available in late 2020.
One theme emerged over the summer—hyping vaccine effectiveness for young children after U.S. authorities authorized and recommended the Pfizer and Moderna shots for children aged 6 months to 5 years.
“We welcome having COVID-19 vaccines to help protect our youngest Marylanders against severe illness, hospitalization, or even death from this virus and strongly encourage parents to vaccinate their children,” Maryland Health Secretary Dennis Schrader said in a statement.
“Clinical trials proved that the pediatric vaccine is an effective way to prevent COVID infection and serious illness in young children,” the Massachusetts Department of Public Health says on its website.
But the clinical trials for the age group weren’t able to measure efficacy against severe illness, which has been acknowledged by the U.S. Centers for Disease Control and Prevention (CDC).
“The clinical trials were not powered to detect efficacy against severe disease in this young population,” Dr. Sara Oliver, a CDC medical officer, told a meeting over the summer.
Saying the vaccines protect young children against severe disease “is a leap of faith,” Dr. David McCune, a hematology and oncology doctor in Washington state, told The Epoch Times. “It’s not supported by the research.”
Officials in every state were asked to provide evidence for dubious or false statements. Maryland officials pointed to a CDC page that did not support Schrader’s statement. Massachusetts officials did not respond to an inquiry.
False Statements on New Boosters
The U.S. Food and Drug Administration (FDA) recently authorized updated booster shots from Moderna and Pfizer. The CDC then recommended them for virtually all Americans aged 12 and older, and later enabled children 5 to 11 to get one of the new shots.
Clinical trials for the bivalent boosters, which contain spike protein components targeting the original COVID-19 strain and the BA.4/BA.4 Omicron subvariants, were not done—and have not been completed—on any group of humans as of yet.
Officials relied on data from testing in mice, data from the original vaccines, and a BA.1/Wuhan bivalent that has never been available in the United States.
The testing on that bivalent, done in adults 18 and older (Moderna) and adults 55 and older (Pfizer), showed that the updated boosters triggered higher levels of antibodies than the old boosters. But the trials didn’t provide any efficacy estimates for protection against infection or severe illness.
The dearth of data didn’t stop states from promoting the vaccines as tools that would definitely work.
“Adding a component to the boosters that specifically targets the subvariants currently circulating will help restore protection against COVID-19 infections, including hospitalizations, that has decreased over time,” Dr. Dean Sidelinger, Oregon’s state epidemiologist, said in a statement.
“The updated bivalent COVID-19 booster, along with the flu vaccine, give parents two powerful tools to protect their children from severe illness and hospitalization,” Dr. Sameer Vohra, the director of the Illinois Department of Public Health, said.
Officials in Oregon and Illinois did not respond to requests for comment.
Minimizing Side Effects
Many states emphasize how most side effects are mild. That’s true, according to data from the CDC and studies. But a number of states fail to mention serious side effects, like heart inflammation, that have been linked to the vaccines.
New York, Pennsylvania, and South Carolina, for instance, didn’t mention myocarditis, a form of heart inflammation, or thrombosis with thrombocytopenia syndrome (TTS), a severe blood clotting issue.
Most of the states that did mention myocarditis promoted the idea that the incidence of myocarditis is higher after COVID-19 infection than after COVID-19 vaccination.
“Myocarditis and pericarditis are much more common if you get sick with COVID-19,” the Washington state Department of Health says on its website.
“The risk of developing myocarditis after a COVID-19 infection is much higher than the risk of developing myocarditis after the vaccine,” the Alabama Department of Public Health said in a press release over the summer.
But more papers show a higher rate of myocarditis after vaccination in high-risk groups, especially young men, including one provided by authorities in Alabama.
Asked for evidence for its statement, Alabama officials sent a link to a British study published after its release was issued. But the study detected a higher risk for young males, or men aged younger than 40 years old, after vaccination.
After that was pointed out, Alabama officials stopped responding.
Some states, like Oregon, say no deaths have been linked to myocarditis after COVID-19 vaccination. Researchers around the world, including with the CDC, have determined there’s a causal link between myocarditis and the Pfizer and Moderna vaccines, which both utilize messenger RNA (mRNA) technology. And autopsies and medical records have confirmed deaths from myocarditis among the vaccinated.
Florida and othercountriesrecommend against or don’t advise messenger RNA vaccination, or the Moderna and Pfizer vaccines, for some age groups due to myocarditis.
TTS is an often-fatal form of blood clotting that happens on occasion after receipt of the Johnson & Johnson vaccine, according to federal officials. The FDA restricted the Johnson & Johnson vaccine due to TTS.
Dr. Danice Hertz, who was injured by a vaccine, says that the statements underline her experience with the health care system and top federal officials. That includes the FDA not acknowledging how many Americans have actually been injured by one of the shots.
“I blame the FDA and our federal government for creating this environment where doctors don’t know anything about vaccine injuries,” she said.
Outdated Information
A number of states still cite data from 2021 or even 2020, even though over half a dozen new variants have emerged since COVID-19 first appeared.
“FDA-authorized COVID-19 vaccines protect against Delta and other known variants,” the Oklahoma State Department of Health says on its website.
The Delta variant stopped circulating in the United States in 2021.
Oklahoma also says that so-called breakthrough cases, or post-vaccination infections, “happen in only a small percentage of vaccinated people.”
That hasn’t been true since Omicron displaced Delta in late 2021.
The California Department of Public Health links to a study from the CDC that was published in August 2021 when claiming that unvaccinated people who already had COVID-19 “are more than twice as likely as vaccinated people to get it again.”
Studies from late 2021and2022 show that post-infection protection, known as natural immunity, is superior to vaccination. Natural immunity has also held up better, but also waned against newer variants.
Heavy Reliance on the CDC
Nearly all of the state health agencies rely heavily on the CDC and other federal agencies.
Many repeatedly reference the CDC on their websites. The CDC has promoted misinformation on COVID-19 vaccines during the pandemic, including the unsupported claim that the vaccines protect young children against severe illness and promoting a study that exaggerated the COVID-19 death toll among children.
States that did provide evidence to back claims mostly cited CDC studies and documents.
The CDC publishes a quasi-journal called the Morbidity and Mortality Weekly Report. The CDC has said (pdf) the publication is distinct from “all other health-related publications,” in part because the content “constitutes the official voice” of the CDC and because most articles are not peer-reviewed. Instead, multiple levels of CDC officials review a submission.
“By the time a report appears in MMWR, it reflects, or is consistent with, CDC policy,” the CDC said in one overview of the publication.
The CDC and its partner, the FDA, have aggressively promoted vaccination during the pandemic, even when little evidence supports the vaccines. The agencies have also repeatedly refusedto releaseCOVID-19 vaccinesafety data.
Dr. Todd Porter, a pediatrician in Illinois, said that the effort to get virtually all children vaccinated against COVID-19, despite the small amount of efficacy and safety data, is contributing to parents hesitating over other vaccines.
“This has created a much different conversation with parents of my patients with respect to benefit/harm and has further eroded parent confidence in public health and has made it harder for me to make recommendations for other more important proven vaccines,” Porter told The Epoch Times in an email. “Most notable has been lack of influenza vaccine uptake in my patients over the past year.”
Steps Forward
Regaining people’s trust is key to moving forward and involves acknowledging information that was conveyed is not correct, experts said.
“When a public health authority or federal official says something that’s incorrect, it has a responsibility to correct it. And when it doesn’t, when it just lets the matter lie, people continue to distrust them even more,” Bhattacharya said.
One example, he said, is how officials repeatedly said—and some are still saying—that the vaccines cut down on transmission, even though a top Pfizer executive recently acknowledged testing on transmission has not been done. The claim that vaccines curb transmission helped lead to vaccine mandates.
“I think it would go a long way if our nation’s public health institutions could demonstrate humility and acknowledge that in the panic of the pandemic they got it wrong where it comes to children,” Porter said.
The urge to get people vaccinated has led to some of the false and misleading claims, according to McCune, who saw the same pattern repeated during the rollout of the new boosters.
“You could have started with the bivalent booster and said, ‘this is what we know. We know some things about antibody levels from basic science studies that were done in animal models and from similar vaccines that were given to humans that we have a reason to believe these antibodies are going to improve,’” he said. “And then to say, ‘the reason we were approving this is we think that this has overall been a safe program, and we don’t anticipate there’ll be future problems. We’re making a leap here to try and get ahead of it, even though there’s some uncertainty.’ That’s an honest statement, but it’s not a very salesy statement.”
Sovereign’s Handbook by Johnny Liberty (30th Anniversary Edition) (3-Volume Printed, Bound Book or PDF)
A three-volume, 750+ page tome with an extensive update of the renowned underground classic ~ the Global Sovereign’s Handbook. Still after all these years, this is the most comprehensive book on sovereignty, economics, law, power structures and history ever written. Served as the primary research behind the best-selling Global One Audio Course. Available Now!
Dawning of the Corona Age: Navigating the Pandemic by Johnny Freedom (3rd Edition) (Printed, Bound Book or PDF)
This comprehensive book, goes far beyond the immediate impact of the “pandemic”, but, along with the reader, imagines how our human world may be altered, both positively and negatively, long into an uncertain future. Available Now!