Let’s focus on the future, and fix the problems we still need to solve.
In April 2020, with nothing else to do, my family took an enormous number of hikes. We all wore cloth masks that I had made myself. We had a family hand signal, which the person in the front would use if someone was approaching on the trail and we needed to put on our masks. Once, when another child got too close to my then-4-year-old son on a bridge, he yelled at her “SOCIAL DISTANCING!”
These precautions were totally misguided. In April 2020, no one got the coronavirus from passing someone else hiking. Outdoor transmission was vanishingly rare. Our cloth masks made out of old bandanas wouldn’t have done anything, anyway. But the thing is: We didn’t know.
I have been reflecting on this lack of knowledge thanks to a class I’m co-teaching at Brown University on COVID. We’ve spent several lectures reliving the first year of the pandemic, discussing the many important choices we had to make under conditions of tremendous uncertainty.
Some of these choices turned out better than others. To take an example close to my own work, there is an emerging (if not universal) consensus that schools in the U.S. were closed for too long: The health risks of in-school spread were relatively low, whereas the costs to students’ well-being and educational progress were high. The latest figures on learning loss are alarming. But in spring and summer 2020, we had only glimmers of information. Reasonable people—people who cared about children and teachers—advocated on both sides of the reopening debate.
Another example: When the vaccines came out, we lacked definitive data on the relative efficacies of the Johnson & Johnson shot versus the mRNA options from Pfizer and Moderna. The mRNA vaccines have won out. But at the time, many people in public health were either neutral or expressed a J&J preference. This misstep wasn’t nefarious. It was the result of uncertainty.
Obviously some people intended to mislead and made wildly irresponsible claims. Remember when the public-health community had to spend a lot of time and resources urging Americans not to inject themselves with bleach? That was bad. Misinformation was, and remains, a huge problem. But most errors were made by people who were working in earnest for the good of society.
Given the amount of uncertainty, almost every position was taken on every topic. And on every topic, someone was eventually proved right, and someone else was proved wrong. In some instances, the right people were right for the wrong reasons. In other instances, they had a prescient understanding of the available information.
The people who got it right, for whatever reason, may want to gloat. Those who got it wrong, for whatever reason, may feel defensive and retrench into a position that doesn’t accord with the facts. All of this gloating and defensiveness continues to gobble up a lot of social energy and to drive the culture wars, especially on the internet. These discussions are heated, unpleasant and, ultimately, unproductive. In the face of so much uncertainty, getting something right had a hefty element of luck. And, similarly, getting something wrong wasn’t a moral failing. Treating pandemic choices as a scorecard on which some people racked up more points than others is preventing us from moving forward.
We have to put these fights aside and declare a pandemic amnesty. We can leave out the willful purveyors of actual misinformation while forgiving the hard calls that people had no choice but to make with imperfect knowledge. Los Angeles County closed its beaches in summer 2020. Ex post facto, this makes no more sense than my family’s masked hiking trips. But we need to learn from our mistakes and then let them go. We need to forgive the attacks, too. Because I thought schools should reopen and argued that kids as a group were not at high risk, I was called a “teacher killer” and a “génocidaire.” It wasn’t pleasant, but feelings were high. And I certainly don’t need to dissect and rehash that time for the rest of my days.
Moving on is crucial now, because the pandemic created many problems that we still need to solve.
Student test scores have shown historic declines, more so in math than in reading, and more so for students who were disadvantaged at the start. We need to collect data, experiment, and invest. Is high-dosage tutoring more or less cost-effective than extended school years? Why have some states recovered faster than others? We should focus on questions like these, because answering them is how we will help our children recover.
Many people have neglected their health care over the past several years. Notably, routine vaccination rates for children (for measles, pertussis, etc.) are way down. Rather than debating the role that messaging about COVID vaccines had in this decline, we need to put all our energy into bringing these rates back up. Pediatricians and public-health officials will need to work together on community outreach, and politicians will need to consider school mandates.
The standard saying is that those who forget history are doomed to repeat it. But dwelling on the mistakes of history can lead to a repetitive doom loop as well. Let’s acknowledge that we made complicated choices in the face of deep uncertainty, and then try to work together to build back and move forward.
Sovereign’s Handbook by Johnny Liberty (30th Anniversary Edition) (3-Volume Printed, Bound Book or PDF)
A three-volume, 750+ page tome with an extensive update of the renowned underground classic ~ the Global Sovereign’s Handbook. Still after all these years, this is the most comprehensive book on sovereignty, economics, law, power structures and history ever written. Served as the primary research behind the best-selling Global One Audio Course. Available Now!
Dawning of the Corona Age: Navigating the Pandemic by Johnny Freedom (3rd Edition) (Printed, Bound Book or PDF)
This comprehensive book, goes far beyond the immediate impact of the “pandemic”, but, along with the reader, imagines how our human world may be altered, both positively and negatively, long into an uncertain future. Available Now!
New evidence has emerged that the mRNA COVID-19 vaccines are routinely injuring the heart of all vaccine recipients, raising further questions about their safety and their role in the recent elevated levels of heart-related deaths.
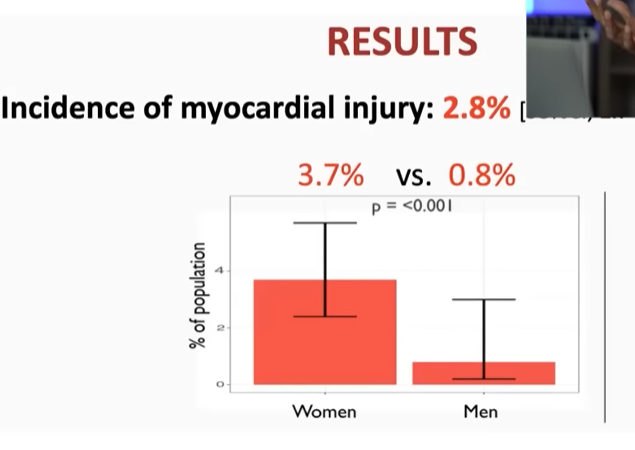
The latest evidence comes in a study from Switzerland, which found elevated troponin levels – indicating heart injury – across all vaccinated people, with 2.8% showing levels associated with subclinical myocarditis.
The official line on elevated heart injuries and deaths, where they are acknowledged, is that they are most likely caused by the virus as a post-Covid condition rather than the vaccines.
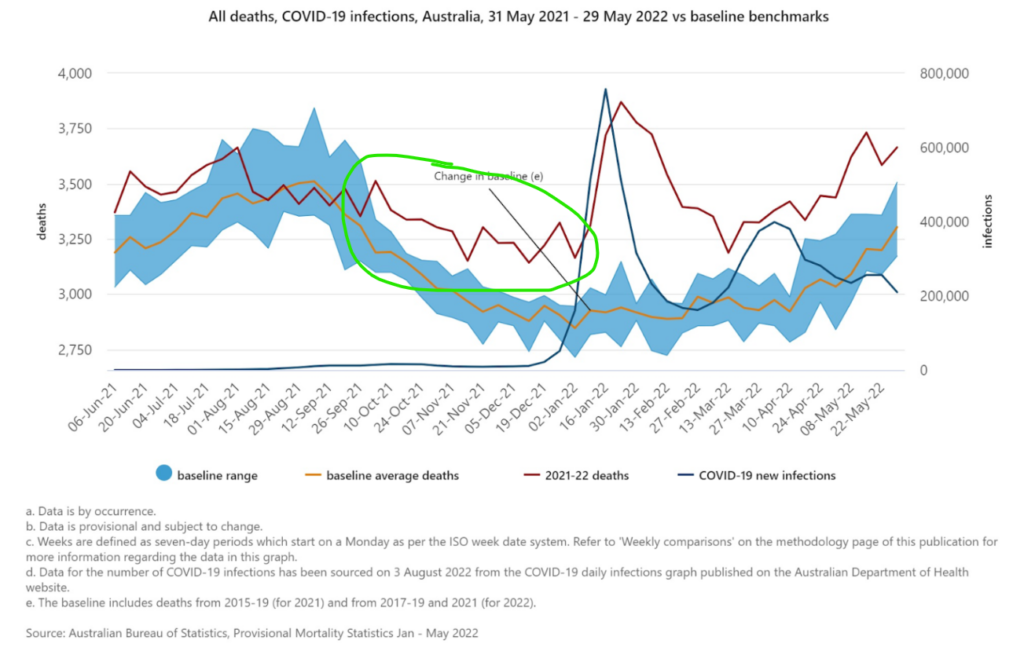
However, expert group HART (Health Advisory and Recovery Team) has pointed to Australia as a “control group” on this question. HART notes that even though Australia had not had significant Covid (only 30,000 reported infections and 910 deaths) prior to mid-2021, it still saw a trend in excess non-Covid deaths beginning in June 2021 (see below). HART notes that Australia “did not have prior Covid as a reason for seeing this rise in mortality and hospital pressure from spring 2021”. Instead, “the results from this control group indicate that the cause of this rise in deaths, particularly in young people, must be something in common with Australia, Europe and the USA”.
Australian Government graph of mortality including Covid mortality. Note the Government chose to plot Covid infections rather than Covid deaths on this chart.
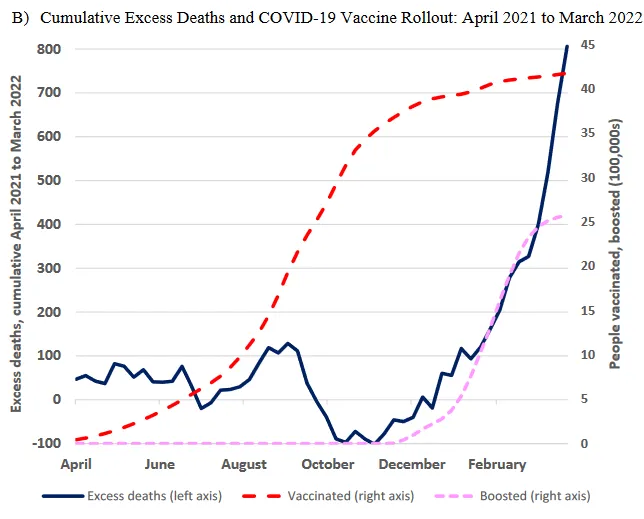
In New Zealand, economist John Gibson found a temporal association between boosters and excess deaths, estimating “16 excess deaths per 100,000 booster doses” (see below). He noted that the age distribution of the deaths corroborated the hypothesis: “The age groups most likely to use boosters show large rises in excess mortality after boosters are rolled out.”
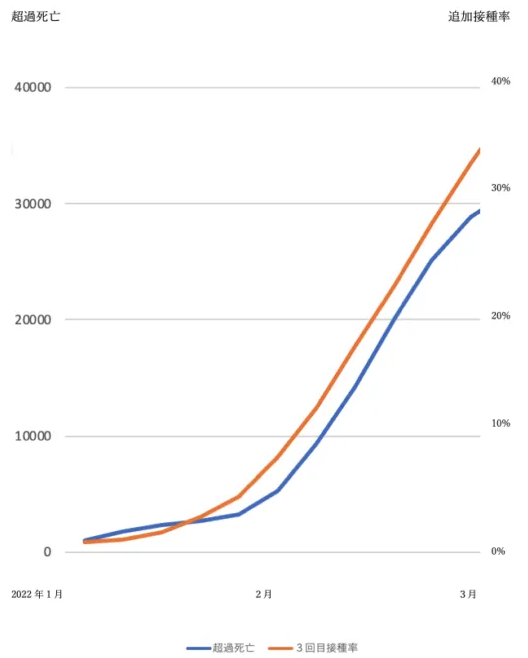
In Japan, Guy Gin reports that Professor Seiji Kojima of Nagoya University found the same correlation during the booster rollout in January to March 2022 (see below) – a time when most excess deaths were not with Covid.
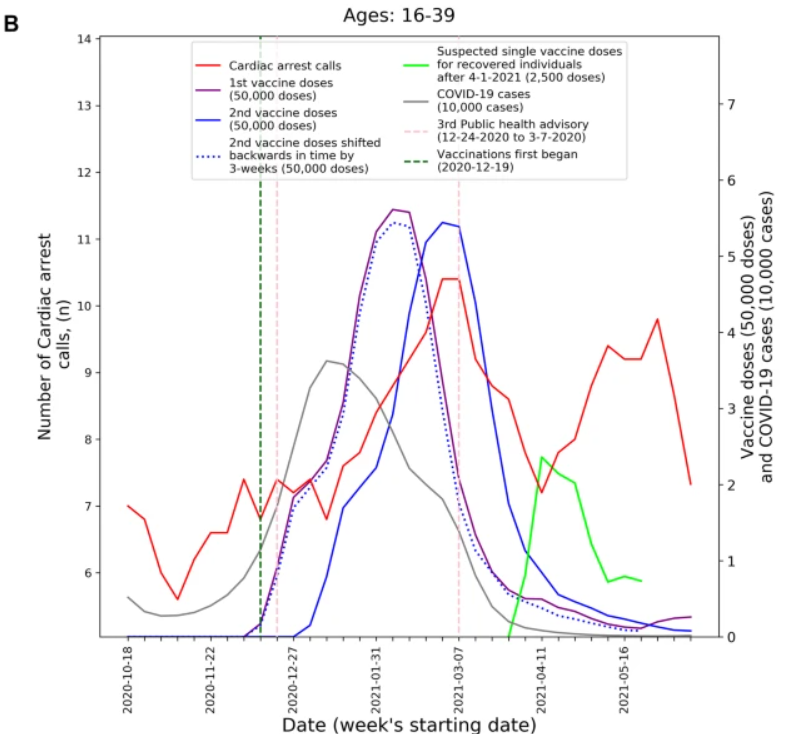
In Israel, a study in Natureobserved a similar trend for 16-39 year-olds, with cardiac arrest emergency calls rising and falling with the first and second doses and then rising and falling again after doses for recovered individuals.
Dr. Eyal Shahar looked at the Israeli deaths data for all ages and estimated “a plausible range of the booster fatality rate in Israel in August 2021” of eight to 17 deaths per 100,000 vaccinees. In the Netherlands, vaccinologist Dr. Theo Schetters estimated a booster fatality rate in the over-60s as high as 125 per 100,000 vaccinees.
As to cause, Dr. Michael Palmer and Dr. Sucharit Bhakdi at Doctors for Covid Ethics have set out what they deem “irrefutable proof of causality” that mRNA vaccines are causing vascular and organ damage. From studies and autopsy evidence the medical experts show:
mRNA vaccines don’t stay at the injection site but instead travel throughout the body and accumulate in various organs;
mRNA-based Covid vaccines induce long-lasting expression of the SARS-CoV-2 spike protein in many organs;
Vaccine-induced expression of the spike protein induces autoimmune-like inflammation;
Vaccine-induced inflammation can cause grave organ damage, especially in vessels, sometimes with deadly outcome.
They explain that autopsy evidence shows that “the strong expression of spike protein in heart muscle after vaccination correlates with significant inflammation and tissue destruction”. They add that “vaccine-induced vascular damage will promote blood clotting, and clotting-related diseases such as heart attack, stroke, lung embolism are very common in the adverse events databases”.
A recent case report in Vaccines of an autopsy conducted on a 76-year-old man who died three weeks after receiving his third COVID-19 vaccination confirms the role of the vaccine. It found the presence of spike protein but not the nucleocapsid protein in the deceased man’s brain and heart, proving that the vaccine (which unlike the virus only produces the spike protein) was the cause of the deadly inflammation.
In the heart, signs of chronic cardiomyopathy as well as mild acute lympho-histiocytic myocarditis and vasculitis were present. Although there was no history of COVID-19 for this patient, immunohistochemistry for SARS-CoV-2 antigens (spike and nucleocapsid proteins) was performed. Surprisingly, only spike protein but no nucleocapsid protein could be detected within the foci of inflammation in both the brain and the heart, particularly in the endothelial cells of small blood vessels. Since no nucleocapsid protein could be detected, the presence of spike protein must be ascribed to vaccination rather than to viral infection. The findings corroborate previous reports of encephalitis and myocarditis caused by gene-based COVID-19 vaccines.
A case report of the autopsy of a 55-year-old patient who died four months after receiving a Pfizer jab as a second dose (his first dose was AstraZeneca) made similar findings.
SARS-CoV-2 Spike protein, but not nucleocapsid protein was sporadically detected in vessel walls by immunohistochemical assay. The cause of death was determined to be acute myocardial infarction and lymphocytic myocarditis. These findings indicate that myocarditis, as well as thrombo-embolic events following injection of spike-inducing gene-based vaccines, are causally associated with a injurious immunological response to the encoded agent.
A recent meta-analysis claimed to find that the risk of myocarditis is “more than seven fold higher in persons who were infected with the SARS-CoV-2 than in those who received the vaccine”. It claims this supports “the continued use of mRNA COVID-19 vaccines among all eligible persons per CDC and WHO recommendations”.
However, critics have pointed out the numerous flaws in this meta-analysis and highlighted that it is at odds with a major Nordic study of 23 million people that found the risk of hospitalisation post-vaccination in 16-24 year old males was up to 28 times higher than the risk post-Covid. At the Daily Sceptic we have written about this Nordic study as well as a number of other studies with similar findings, including ones from France, England and the U.S. (alongside critiques of studies that purport to show otherwise). A study from Israel confirms the elevated risk from vaccination and states: “We did not observe an increased incidence of neither pericarditis nor myocarditis in adult patients recovering from COVID-19 infection.” A study from Italy found a similar absence of elevated myocarditis during the pre-vaccination pandemic period.
We should also note that vaccination does not prevent Covid infection so the risks are additive and the comparison between vaccination risk and infection risk is false. Cardiovascular injury also is not the only serious adverse event associated with these vaccines. A recent study by researchers from Harvard, Oxford and Johns Hopkins University (among others) found that the mRNA vaccines are up to nearly 100 times more likely to cause a person of student age serious injury than prevent him or her from being hospitalised with COVID-19.
Most of these studies only look at clinical adverse events, i.e., events serious enough to warrant medical assistance. Studies are now emerging which show these clinical events to be just the tip of the iceberg of a far larger number of subclinical injuries. A study in Thailand found cardiovascular adverse effects in around a third of teenagers (29.2%) following Pfizer vaccination and subclinical heart inflammation in one in 43 (2.3%).
The Swiss study mentioned above was recently highlighted by Dr. Vinay Prasad and comes from the European Society of Cardiology. It confirms the Thai result, finding at least 2.8% with subclinical myocarditis (possibly more as the researchers excluded half the cases as possibly from another cause). Dr. Prasad observes that this means subclinical myocarditis is hundreds of times (“two orders of magnitude”) more common than clinical myocarditis. The rates were highest in women at 3.7%, which is one in 27 vaccinated. (Dr. Prasad notes this is different to the Thai study, which found the usual higher rates in males; he suggests this may be related to how the researchers excluded cases.)
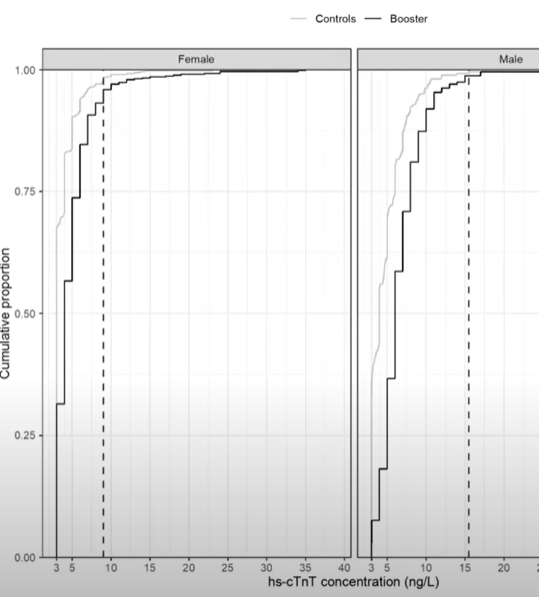
Crucially, the study found elevated troponin levels – indicating heart injury – across all vaccinated people (see chart above, where the dark lines being shifted to the right of the fainter control group lines implies elevated levels throughout the vaccinated population). This indicates the vaccine is routinely injuring the heart (an organ which does not heal well) and that the known injuries are just the more severe instances of a far larger number occurring right across the board.
These injuries are not necessarily short and over with quickly. Studies haveshown that spike protein is still being found in the blood of many vaccinated people at least four months after vaccination, suggesting it is still being produced in some way. The mechanism of this long-term production of spike protein by the body has not been identified (is the genetic code being incorporated into the cell’s DNA?). But if cells in the cardiovascular system and elsewhere are still producing this pathogenic and inflammatory protein for months on end, the risk of auto-immune injury as identified in the autopsies above greatly increases. Such an auto-immune injury may be triggered by re-challenge by the virus ramping up the immune response to the spike protein, which may explain why excess non-Covid deaths often accompany Covid waves.
There is now considerable evidence that mRNA vaccines are routinely injuring the heart, with raised troponin levels across the board and subclinical myocarditis in up to one in 27 cases or more. These are not rare events, as is often claimed by medical authorities and in the media. They are alarmingly common.
Sovereign’s Handbook by Johnny Liberty (30th Anniversary Edition) (3-Volume Printed, Bound Book or PDF)
A three-volume, 750+ page tome with an extensive update of the renowned underground classic ~ the Global Sovereign’s Handbook. Still after all these years, this is the most comprehensive book on sovereignty, economics, law, power structures and history ever written. Served as the primary research behind the best-selling Global One Audio Course. Available Now!
Dawning of the Corona Age: Navigating the Pandemic by Johnny Freedom (3rd Edition) (Printed, Bound Book or PDF)
This comprehensive book, goes far beyond the immediate impact of the “pandemic”, but, along with the reader, imagines how our human world may be altered, both positively and negatively, long into an uncertain future. Available Now!
High pressures could heal the brain after spike protein injury
Hyperbaric oxygen therapy (HBOT) is a treatment that increases blood oxygen levels to boost wound healing and clear bacterial infections. Recent studies and doctors’ clinical experiences suggest that it may be useful for treating long COVID and post COVID vaccine symptoms.
“When I first heard about it [HBOT] I thought, ‘this is goofy,’” said Dr. Paul Marik. Then he encountered a competitive cyclist patient who became bedridden after COVID vaccinations. “He was completely incapacitated. He went for hyperbaric oxygen [and] within about five or six sessions [he] was back on his bicycle.”
Marik, co-founder of the Front Line COVID-19 Critical Care Alliance (FLCCC), told The Epoch Times, that some patients who have spike protein injuries have responded particularly well to hyperbaric oxygen.
Epigenetics are factors that change gene activity. Depending on environmental factors including stress, diet, drugs, and treatments, certain genes can be activated or suppressed.
“Surprisingly, it is the increased pressure, rather than the increase in the concentration of dissolved oxygen, that appears to mediate these effects,” the FLCCC doctors wrote in their treatment recommendations.
For HBOT, the higher the oxygen pressure, the greater the change in gene expression, and the higher the general benefit.
Therefore the FLCCC recommends to use HBOT at a high atmospheric pressure. But treatment regimens need to be monitored by a clinician to prevent oxygen toxicity.
An in vitro study on human microvascular cells found that cells exposed to a HBOT treatment at 2.4 standard atmospheres (ATM) for 60 minutes, had changes in gene expression in 8,101 genes 24 hours later.
HBOT increased the expression of anti-inflammatory genes and reduced the activity of pro-inflammatory genes.
Since cells exposed to pure oxygen at normal atmospheric pressure had “minimal change” in their gene expression, this demonstrated that pressure is the key player in the overall therapy.
Another study on rats further indicated the importance of pressure. The study showed that depending on the pressure of the environment, different numbers of genes were expressed.
The authors of the study exposed rats to normal air and pure oxygen at normal atmospheric pressure and higher pressures. The data showed that in rats, as oxygen levels increased from the pressure would cause an increase in gene expression.
Studies showed that HBOT could reduce inflammatory pathways and reduce the action of pro-inflammatory toll-like receptor pathways, both of which are often activated in acute COVID infections and spike protein-induced diseases.
Mitochondria are responsible for breaking down the sugar we ingested through our food, into energy, and uses oxygen as a key reactant of this biochemical process.
During inflammation experienced in long COVID and post-vaccine syndromes, the spike protein can stress the mitochondria in the cell, leading to reduced energy production and more production damaging radical species. Therefore the extra oxygen provided through the treatment gives ample material for use by the mitochondria to increase energy production for the body.
HBOT also induces the release of stem cells and tissue growth factors.
Many studies found the treatment to be beneficial in promoting tissue regeneration including the regeneration of muscle cells and generation of new blood vessels, this indicates that HBOT can help in the repair of tissue damaged from spike protein injuries.
Neurological symptoms are some of the major symptoms in long COVID and post-vaccine symptoms. There are also studies that showed that HBOT enhanced neurogenesis, though HBOT has not been approved by the Foods and Drug Administration for such treatment yet.
Harch has had successes in treating wounds in the brain including a near-reversal of brain damage in a drowned 2-year-old girl in 2017.
The girl had suffered from a deep brain injury and had “no speech, gait or responsiveness to commands with constant squirming and head shaking” he said.
But following 40 sessions, the girl had near-normal motor function, normal cognition, gait, and temperament, and improvement on nearly all neurological exam abnormalities. Her speech improved to a greater level than pre-drowning and she also discontinued all of her medications, according to the LSU Health New Orleans School of Medicine media release.
Studies have also found HBOT treatments increased blood flow and induced microstructural changes; this led to improved brain function including cognitive functions, gait, and sleep.
Studies on HBOT therapies have shown it to be beneficial against COVID and long COVID. There is much literature on HBOT that find positive outcomes in treating COVID infections.
All of the COVID patients presented low oxygen levels, rapid breathing, and inflammatory markers. After one to six sessions of HBOT, inflammatory markers fell and the rapid breathing ceased.
“Most importantly, HBOT potentially prevented the need for mechanical ventilation,” the authors wrote.
In a randomized controlled study from Argentina, HBOT was used to treat for low oxygen in COVID-19. The study was stopped after the interim analysis of 40 patients’ outcomes. The differences between the treatment and the non-treatment group were obvious.
Patients under treatment for HBOT improved their blood oxygen levels in three days, compared to the non-treatment group which took 9 days.
In particular, studies on long COVID showed that HBOT has significant improvements on fatigue, and brain fog by improving attention, memory, information processing, and mental health.
In an Israeli study published in July 2022 on 73 long COVID patients, half (37) were treated with HBOT and the other half (36) with placebo. The patients received treatments five times a week and the protocol included breathing pure oxygen by mask at 2 ATM for 90 minutes.
The authors noticed improvements in the HBOT treatment group in global cognitive function, attention, and executive function, with significant improvements in energy, sleep, mental health, and reduced pain.
Brain scans of these patients further showed improved blood flow in certain areas of the brain, suggestive of blood vessel formation.
The FLCCC recommends HBOT as a third line treatment as it is considered to be a treatment that “may be lifesaving for one patient and totally ineffective for another,” and is therefore less applicable for the general population.
Marik also acknowledged that the high cost of the therapy and differences in pathophysiology may not make the treatment suitable for everyone. They currently recommend HBOT only for severe neuropathologies in patients suffering from post-vaccine syndromes, particularly peripheral neural pain. Contraindications for this treatment include people with untreated pneumothorax.
Sovereign’s Handbook by Johnny Liberty (30th Anniversary Edition) (3-Volume Printed, Bound Book or PDF)
A three-volume, 750+ page tome with an extensive update of the renowned underground classic ~ the Global Sovereign’s Handbook. Still after all these years, this is the most comprehensive book on sovereignty, economics, law, power structures and history ever written. Served as the primary research behind the best-selling Global One Audio Course. Available Now!
Dawning of the Corona Age: Navigating the Pandemic by Johnny Freedom (3rd Edition) (Printed, Bound Book or PDF)
This comprehensive book, goes far beyond the immediate impact of the “pandemic”, but, along with the reader, imagines how our human world may be altered, both positively and negatively, long into an uncertain future. Available Now!
More than 18 million people were injured so badly by their first COVID shot from Pfizer or Moderna that they had to go to the hospital. That’s according to the CDC’s own internal data, which a court just ordered the federal agency to release to a watchdog group.
Instead of alerting the public to the incredible dangers of these shots and completely shutting down Joe Biden’s mass vaccination mandates, the CDC covered up the info until it was forced to release. Everyone in a position of authority at the CDC should be fired for this. What good is a “public health” agency if it fails to alert the public that 8% of vaccine recipients are being hospitalized?
The CDC started a vaccine monitoring program back at the very beginning of the COVID shot rollout in December of 2020. You might remember it. The program was called V-safe. People were asked to install the V-safe app on their smartphones and then self-report if they have any negative effects from the experimental mRNA shots, which were released to the public under an Emergency Use Authorization from the FDA.
A lot of people were eager to help, because world governments had scared many folks very badly over the virus. Many thought that the COVID shots were a medical miracle in late 2020. So, more than 10 million people downloaded V-safe on their smartphones, and then proceeded to get vaccinated.
That’s a huge sample size for a medical study. With 10 million people participating in the V-safe self-reporting system, it gives us an extremely accurate statistical model to use when studying the 230 million Americans who have had at least one COVID shot.DC
The CDC tracked data in the V-safe program for the first 18 months of the vaccine’s public availability, up through July of this year. But then, strangely, the CDC never published any data from V-safe. We couldn’t see it. We just had to trust the CDC, which had been caught lying repeatedly.
The CDC’s main webpage about the mRNA COVID shots still says, to this very day, “COVID-19 vaccines are safe, effective and free.” That’s the very first sentence on the website. Safe and effective! That’s been the CDC’s position for the entire time. The vaccines are safe, and they cannot hurt you.
If that’s true, then why wouldn’t the CDC release the data until a court ordered it to do so following a lawsuit by the Informed Consent Action Network (ICAN)? The data speaks for itself.
Of the 10 million people who participated in V-safe – again, a massive sample size – 3.3 million reported Adverse Health Impacts (AHIs) immediately after their first vaccination. That’s 33% or one-in-three. Of those 3.3 million people, 1.2 million reported that they were unable to perform daily activities for a time after vaccination. 1.3 million reported getting so sick from the shots that they had to miss school or work. And about 800,000 reported being hospitalized by their COVID vaccination.
That last figure is the most worrisome. 800,000 hospitalizations out of 10 million people? That’s an 8% hospitalization rate. It means that as many as 18 million of the 230 million people who received at least one shot may have been hospitalized with an adverse reaction.
A study published in June of 2021 by the National Institutes of Health – where Tony Fauci works – found that the hospitalization rate from COVID-19 for the total population was 2.1%. If you are under the age of 40, the hospitalization rate from COVID-19 is just 0.4%.
For the shots, the hospitalization rate has been 8%.
This means that:
YOU ARE 4 TIMES AS LIKELY TO BE HOSPITALIZED BY THE VACCINES THAN BY COVID ITSELF, NO MATTER WHAT AGE GROUP YOU ARE IN.
YOU ARE 20 TIMES AS LIKELY TO BE HOSPITALIZED BY THE SHOTS IF YOU ARE UNDER AGE 40 THAN BY COVID ITSELF.
ICAN has set up a website where you can finally view the CDC’s V-safe data online. The data was released on October 3, 2022, under a court order. You can see the data for yourself HERE.
The CDC has been lying to the American people about the vaccines all this time. There need to be legal consequences for this. Public trials and long jail sentences are necessary for anyone at the CDC who participated in this cover-up.
Sovereign’s Handbook by Johnny Liberty (30th Anniversary Edition) (3-Volume Printed, Bound Book or PDF)
A three-volume, 750+ page tome with an extensive update of the renowned underground classic ~ the Global Sovereign’s Handbook. Still after all these years, this is the most comprehensive book on sovereignty, economics, law, power structures and history ever written. Served as the primary research behind the best-selling Global One Audio Course. Available Now!
Dawning of the Corona Age: Navigating the Pandemic by Johnny Freedom (3rd Edition) (Printed, Bound Book or PDF)
This comprehensive book, goes far beyond the immediate impact of the “pandemic”, but, along with the reader, imagines how our human world may be altered, both positively and negatively, long into an uncertain future. Available Now!
So much basic scientific data and so many best practices and ethical standards in public health were abandoned during the Covid pandemic, it would be difficult to list them all.
Nevertheless, we must remember just how much reality has been warped since March 2020 and try to understand how that warping occurred. Maybe if we understand what happened, we can prevent it from happening again. Maybe we can unwarp the narrative enough so that more people can see clearly what went wrong.
For my own sanity, I need to understand what happened, so I can come to terms with why people behaved the way they did, and why so many of my own assumptions were shattered during the pandemic.
I want to know why real science got thrown out as misinformation, propaganda turned into absolute truth, the free press morphed into a government mouthpiece, and supposedly liberal and scientific institutions abandoned ethical standards and critical thought to impose zero-evidence, zero-Covid authoritarian lockdowns and mandates.
How did my family, friends and neighbors – who I thought shared my liberal, humanist values – turn into a group-thinking, bullying herd? What forces were exerted to erase scientific and intellectual integrity from the minds of literally millions of doctors, scientists, economists, journalists, educators and other normally curious and compassionate people worldwide?
To answer these questions, I am less interested in an exact timeline than in a story that makes sense of seemingly senseless behaviors. I am also less interested in the culpability of specific individuals than in an examination of the factors – psychological, social, historical, political – that drove those behaviors.
Overall, I believe four extremely powerful forces converged catastrophically to initiate, and then perpetuate, the snowball that became the avalanche of Covid insanity. And by insanity, I mean the imposition of unprecedented, untested and predictably unsuccessful – not to mention horrifically damaging – pandemic containment measures.
Those four forces were: panic, politics, propaganda, and profits.
Panic
I believe pandemic panic was driven from above – from the highest echelons of the most powerful governments – and below – within populations primed for disaster and perpetually on the verge of a nervous breakdown.
Panic from above: it had to be a lab leak
The stratospheric level of panic unleashed over a virus of relatively low lethality (estimated overall infection fatality rate <0.2%) has always seemed wildly disproportionate to me. When previous, muchmore lethal viruses were discovered in various populations, nothing near the level of Covid hysteria happened.
I therefore surmise that, at the onset of the Covid pandemic, there was a spark of panic from a very powerful place that ignited the fear already smoldering in the population.
Much has been written about the lab leak hypothesis in terms of detailed timelines and specific people involved. To me, the most compelling argument in its favor is psychological: Without the lab leak there would be insufficient momentum to fuel such a juggernaut of global panic, causing scientists and public health experts to abandon everything they knew about respiratory viruses, and leading democratic governments to adopt Chinese-inspired authoritarian policies.
Specifically, the Wuhan lab leak makes sense as the source of initial panic because the research conducted there is highly sensitive and controversial. It involves EPPPs – enhanced pandemic potential pathogens – viruses engineered to be very contagious so their spread can be studied in animal models. Interest in this type of research comes not just from the virology and epidemiology fields, but also from national security and intelligence agencies focused on bioterrorism.
If both public health and intelligence officials knew, or suspected, that a virus had leaked from a lab studying EPPPs, there would be huge levels of apprehension, not to say hysteria, in that group, even if initial data showed, as it did, that the virus was not very dangerous to most people and affected mostly those over 65 with multiple underlying conditions.
If the virus was intentionally engineered for its pandemic-causing potential, it could be way more dangerous than just any old pathogen jumping from animals to humans. Who knew how an engineered virus would evolve? How much more virulent could it become? Intelligence and national security officials, in particular, might push for a maximal response without reference to standard epidemiologic or public health protocols.
In fact, it is almost impossible to explain the drastic abandoning of everything scientists and public health practitioners knew and believed about flu-like pandemics, without adding to the equation the terrifying unknown of what an engineered pathogen might do.
And to top off the panic palooza, if and when the truth of the virus’s origins came out, those involved with the EPPP research, already riddled with safety concerns, would be blamed. Major international and diplomatic crises could ensue.
Further strengthening this hypothesis is the fact that the countries with the strictest and most prolonged lockdowns, including Australia, New Zealand and Canada, were all members of the “Five Eyes” intelligence alliance, along with the US and UK. It makes sense that precisely those countries sharing the earliest and most detailed intelligence about the lab leak felt not only justified, but compelled, to carry out the strictest lockdowns.
All of this leads me to conclude that a small group of top intelligence and public health officials, fearing a catastrophically deadly engineered virus had been released (regardless of its observed effects in the real world), convinced themselves, their governments, and in turn their populations (without publicly revealing the virus’ origin) that the strictest containment measures were needed or else millions would die.
Panic, then, became not just a reaction to the virus but, in the minds of those instigators, a necessary state in which to hold the population in order to elicit maximum compliance with containment measures. As inertia set in following the big initial push, panic and compliance became not just means for supposedly ending the pandemic but goals in and of themselves.
Scientists and media enlisted in panic campaign
All major media outlets, including the billionaire owners of the largest social media platforms, were likely asked by panicked government officials for their help in supporting draconian virus-suppressing measures. It seems likely, based on the strict adherence to the panic narrative, that guidelines were disseminated as to how the pandemic should be discussed, warning that any deviation therefrom would lead to countless unnecessary deaths. The threat of the virus could not be overstated. Questioning anti-virus measures was taboo.
Although prominent epidemiologists and public health experts outside the inner circle tried to publicize alternative, more realistic scenarios, based on data already gathered about the virus’s actual fatality rates, I believe the government’s allies in academia – some perhaps apprised of the EPPP situation, some politically motivated and/or petrified by the propaganda (as discussed below) – brutally silenced any discussion or debate.
Panic from below: the madness of crowds
The US population was primed to react strongly when massive panic from above was unleashed upon it. Covid fears had already been building since early 2020, with the proliferation of terrifying videos and reports of people falling dead in China’s streets from a hitherto unknown virus. We now know these videos were most likely fake and related to the Chinese propaganda campaign discussed later in this article. But at the time, they went viral, fomenting fear of the new virus.
Even before that, in the years leading up to the pandemic, especially in liberal coastal cities, a culture of hyper safety and risk aversion had taken hold. It was a perfect setup – in addition to the strong political forces acting on the very same populations (as described below) – for pandemic hysteria to proliferate even more virulently than the pathogen that prompted it.
Once large socioeconomically and politically homogeneous groups embraced the panic, as Gigi Foster, Paul Frijters and Michael Baker so cogently explain, herd mentality, or the madness of crowds, took over. To this day, the crowd madness continues to block any critical analysis or questioning of Covid policies in these groups.
Politics
If the pandemic had not happened during the Trump presidency, the panic from above and below might not have garnered enough scientific and media buy-in to turn the entire Democratic Party, as well as other self-regarding liberal governments around the world, into mirror images of totalitarian authorities they so often decried.
Trump was considered by the politically left-leaning coastal elites in the US (myself included!), and their allies around the world, to be a menace the likes of which had never been elected before, and a clear and present danger to the very foundations of democracy. For over three years, these groups, largely controlling the mainstream marketplace of ideas, spent much of their time ridiculing, lambasting and whipping up fear of Trump’s incompetence and nefarious intentions.
Like many others on all sides of the political spectrum, I believe criticism of Trump was largely justified. However, for many Democrats, Trump hatred went beyond rational debate and came to dominate not just the discourse but the very identity of the party, fostering a self-righteous superiority complex displayed through ritualistic virtue signaling, and engendering the apt label “Trump derangement syndrome.” The derangement part was the turning of anti-Trumpism into a self-identifying obsession and singular standard of virtue, to the exclusion of any objective examination of Trump’s words or deeds.
Anything Trump said, the anti-Trump camp felt it their civic and moral duty not just to proclaim, but to deeply believe, the opposite.
When it came to the pandemic, this meant that:
If Trump warned that prolonged lockdowns would wreck the economy, left-leaning economists derided anyone who, as they myopically contended, put economic concerns over human life.
If Trump claimed children were immune to the virus, every Democrat was convinced it would kill their own children and everyone else’s, and that schools should be closed indefinitely.
If Trump said masks don’t work, doctors who for years had known masks to be useless at blocking transmission of flu-like viruses, now believed masks should be mandated everywhere forever.
If Trump suggested that the virus came from a lab in China, editorial boards at major newspapers believed this must be a racist smear which should never ever be entertained, let alone investigated.
And, in my personal life, if I tried to share data showing Covid was not very lethal or that mask mandates did not work, instead of discussing the merits of the data, my friends (who knew very well my ultra-leftie politics and socialist worldview) would turn to me in horror and ask: “Are you a Trumpist?”
Thus was Trump derangement syndrome seamlessly transmuted into Covid derangement syndrome. All the rage directed at Trump was redirected toward anyone who, like Trump, dared to doubt its deadliness or question the authoritarian measures used to fight it.
To top it all off, the pandemic happened during an election year. So Trump hatred and pandemic hysteria were effectively bundled together to get Trump voted out and Biden, a Democrat more aligned with the public health establishment, in. Subsequently, anyone elected on a pro-lockdown, zero-Covid agenda was incentivized to continue advocating for the strictest measures for as long as possible.
Although they knew from the experience of past epidemics, and from basic epidemiologic science, that it is not possible to stop the spread of a flu-like virus once it has seeded itself throughout a global population, I think public health and national security officials – especially those in the lab leak group, as described above – desperately wanted to believe that the Chinese measures were working. After all, nothing like that had ever been tried before. If China said it was working for them, maybe it would work everywhere else. It had to work. Otherwise, they feared, millions of people would die and they would be blamed.
Even as months and years passed, and the virus continued to infect every population in every other country, the world continued to believe China’s zero Covid reports. In fact, the scientifically and medically nonsensical “zero-Covid” goal became the mantra for the authorities imposing Chinese-style virus containment measures everywhere else.
Scientists and media successfully propagandized
One very influential part of the effort to freak the world out about Covid was the early modeling provided by the Imperial College of London in early 2020. Not coincidentally, as proudly declared on its own website, Imperial College is one of China’s top academic and research partners in England.
A scientific and journalistic consensus quickly coalesced around these models and the necessity for the zero-Covid measures they supposedly proved. As mentioned above, dissenting views were silenced, but they were also a small minority. The toxic confluence of panic, politics and propaganda worked like an anti-truth potion to preclude even the possibility that someone would think, let alone publicize, anything suggesting it wasn’t as bad as everyone – the Chinese, the US government, the leading newspapers and scientific journals – said it was.
Profits
President Biden took office just as Covid vaccines became available. This was supposed to be the beginning of the end of lockdowns and a return to normal.
Alas, at this point so many profit-driven interests had piled onto the zero-Covid train, that it continued to hurtle forth at unstoppable speeds.
The nonsensical, non-scientific zero-Covid measures that had begun from a place of mortal panic, spread through political polarization, and amplified by Chinese propaganda, now generated unprecedented profits for anyone who made anything related to the pandemic.
As far as these money interests are concerned, the pandemic might as well go on forever.
In assessing the potential influence of profits on the indefinite continuation of the state of Covid emergency, the numbers speak for themselves. Here are just a few of the jaw-dropping reports on the beneficiaries from never-ending Covid:
Big Tech
In October 2021 the New York Times reported: “In the last year, the five tech superpowers — Amazon, Apple, Google, Microsoft and Facebook — had combined revenue of more than $1.2 trillion. … some of the companies are growing faster and are more profitable than they have been in years.”
Test Makers and Sellers
In January 2022 CBS reported “Windfall profits for test makers,” including Abbott Laboratories ($1.9 billion in third-quarter sales related to COVID-19 testing, up 48% compared to the year-ago period). Other beneficiaries with skyrocketing profits were labs that process PCR tests and drugstore chains like CVS and Walgreens.
Vaccines
In February 2022 The Guardian reported that Pfizer made nearly $37 billion in sales from its Covid-19 vaccine in 2021 – making it one of the most lucrative products in history. Pfizer’s overall revenues in 2021 doubled to $81.3 billion, and it expects to make record revenues of $98 – $102 billion this year.
Billionaires
In January 2022 OxFam reported: “The world’s ten richest men more than doubled their fortunes from $700 billion to $1.5 trillion —at a rate of $15,000 per second or $1.3 billion a day— during the first two years of a pandemic that has seen the incomes of 99 percent of humanity fall and over 160 million more people forced into poverty.”
“If these ten men were to lose 99.999 percent of their wealth tomorrow, they would still be richer than 99 percent of all the people on this planet. They now have six times more wealth than the poorest 3.1 billion people.”
Conclusion
An engineered pandemic potential pathogen leaked from a high-security US-funded lab in Wuhan long before it was acknowledged by China. By the time it became known, it was too late to contain.
Having outlined the cataclysmic convergence of forces I believe came together to create the Covid catastrophe, I now have a Covid story that makes sense to me:
When they found out, top US intelligence and public health officials affiliated with the Wuhan research panicked, fearing millions of deaths, international mayhem and personal culpability. This caused them to disregard real-world data about the virus and to abandon basic epidemiological principles and best practices in public health.
The Chinese authorities adopted scientifically nonsensical zero-Covid policies not because they thought they would work but to deflect attention from China’s role in the viral leak and coverup. In a brilliant propaganda coup, they turned the pandemic into a celebration of their authoritarian measures, convincing the world to follow their example.
All Democrats in the US and their allies elsewhere reflexively and uncritically favored all the policies that President Trump – viewed as their mortal enemy – opposed. These were the very same scientifically bogus policies that the panicked officials and Chinese propagandists were pushing.
Many who controlled the narrative in media, academia, public health and medicine were particularly susceptible to panic, politicization of the pandemic, and Chinese propaganda, which all came together to induce widespread groupthink and herd behavior. As cogently explained inThe Great Covid Panic, such behavior is detached from logical reasoning and the ability to objectively evaluate reality.
Major industries and individuals with enormous wealth and influence saw huge gains from the pandemic. It was, and still is, in their best interests to push for more testing, more treating, more vaccinating, more remote work and learning, more online shopping, and more of everything else pandemic-related.
Although terrifying and depressing to the extreme, this story helps me understand how so many people’s views of data, science, truth, ethics and compassion became so warped. I hope the telling will at least help a little with the unwarping.
new scientific study entitled “Serious adverse events of special interest following mRNA vaccination in randomized trials” provides the best evidence yet concerning the safety of the mRNA Covid vaccines. For most vaccines in common use, benefits far outweigh risks, but that may not be the case for the mRNA covid vaccines, according to this study by Joseph Fraiman and his colleagues. It depends on your age and medical history.
The randomized controlled clinical trial is the gold standard of scientific evidence. When regulators approved the Pfizer and Moderna mRNA vaccines for emergency use in December 2020, tworandomized trials showed that the vaccines reduced symptomatic covid infection by over 90% during the first few months after the second dose.
Pfizer and Moderna did not design the trials to evaluate long-term efficacy or the more important outcomes of preventing hospitalization, death, or transmission.
The randomized trials did collect adverse event data, including the presence of mild symptoms (such as fever) and more serious events requiring hospitalization or leading to death. Most vaccines generate some mild adverse reactions in some people, and there were considerably more adverse such reactions after the mRNA vaccines compared to the placebo.
That is annoying but not a major issue. We care about severe health outcomes. The key question is whether the vaccine’s efficacy outweighs the risks of severe adverse reactions.
The Fraiman study uses data from the same Pfizer and Moderna-sponsored randomized trials presented to the FDA for vaccine approval, but with two innovations that provide additional information.
First, the study pools data from both mRNA vaccines to increase the sample size, which decreases the confidence intervals’ size and the uncertainty about the estimated harms.
Second, the study focuses only on the severe adverse events plausibly due to the vaccines. Serious adverse events such as gunshot wounds, suicide, animal bites, foot fractures, and back injury are unlikely to be due to a vaccine, and cancer is unlikely to be due to a vaccine within a few months after vaccination. By removing such random noise, the ability (statistical power) to detect genuine problems increases. If there is no excess risk, shorter confidence intervals bolster confidence in the safety of the vaccines.
Classifying adverse events into the two groups is not a trivial task, but Fraiman et al. do an excellent job to avoid bias. They rely on the pre-defined Brighton Collaboration definitions of adverse events of special interest (AESI). Founded in 2000, the Brighton Collaboration has two decades of experience using rigorous science to define clinical outcomes for vaccine safety studies.
Moreover, Fraiman and colleagues blinded the process where they classified the clinical events as AESIs. Adjudicators did not know whether the individual had received the vaccine or the placebo. Hence, any criticism of so-called p-hacking is unwarranted.
So, what are the results? There were 139 AESIs among the 33,986 people vaccinated, one for every 244 people. That may sound bad, but those numbers mean nothing without comparison against a control group. There were 97 AESIs among the 33,951 people who received a placebo. Combining these numbers implies 12.5 vaccine-induced AESIs for every 10,000 people vaccinated, with a 95% confidence interval of 2.1 to 22.9 per 10,000 people. To phrase it differently, there is one additional AESI for every 800 people vaccinated (95% CI: 437-4762).
That is very high for a vaccine. No other vaccine on the market comes close.
The numbers for the Pfizer and Moderna vaccines are 10 and 15 additional events per 10,000 people, respectively, so both vaccines contributed to the finding. The numbers are similar enough that we cannot confidently say that one is safer than the other. Most excess AESIs were coagulation disorders. For the Pfizer vaccine, there was also an excess of cardiovascular AESIs.
While these safety results are concerning, we must not forget the other side of the equation. Unfortunately, the study does not calculate composite estimates that also included the reduction in serious covid infections, but we have such estimates for mortality.
Dr. Christine Benn and her colleagues calculated a combined estimate of the effect of vaccination on all-cause mortality using the same randomized trial data as Fraiman et al. They did not find a mortality reduction for the mRNA vaccines (relative risk 1.03, 95% CI: 0.63-1.71).
One important limitation of both Fraiman’s and Benn’s studies is that they do not distinguish the adverse reactions by age, comorbidities, or medical history. That is not their fault. Pfizer and Moderna have not released that information, so outside researchers do not have access.
We know that the vaccine benefits are not equally distributed among people since covid mortality is more than a thousand times higher among the old. Thus, risk-benefit calculations must be done separately for different groups: with and without prior covid infection, by age, and for the first two doses versus boosters.
Covid-recovered people have natural immunity that is stronger than vaccine-induced immunity. So, the benefit of vaccination is – at best – minimal. If the risk of adverse reactions is the same as in the randomized trials, there is a negative risk-benefit difference. Why are we mandating people in this group to be vaccinated? It is both unethical and damaging to public health.
While everyone can get infected, children have a minuscule risk of covid mortality. There is very limited safety data from the trials on children. If the risk of adverse reactions is the same as for adults, the harms outweigh the risks. Children should not receive these vaccines.
Older people above 70 have a much higher risk of covid mortality than the population in the Fraiman study. If their risk of adverse reaction is the same, then the benefits outweigh the harms. Hence, older people who have never had covid and are not yet vaccinated may benefit from these vaccines. However, we do not know if they are better than the Johnson & Johnson and Astra-Zeneca vaccines.
It is unclear from the clinical trial data whether the benefits outweigh the risks for working-age adults who have not been vaccinated and who have not already had covid. This is true both historically, for the original covid variants, and currently for the newer ones.
The Fraiman study analyzes data after the first and second doses. Both risks and benefits may differ for booster shots, but no randomized trial has properly evaluated the trade-off.
These results concern only the Pfizer and Moderna mRNA vaccines. Fraiman et al. did not analyze data on the adenovirus-vector vaccines marketed by Johnson & Johnson and Astra-Zeneca. Benn et al. found that they reduced all-cause mortality (RR=0.37, 95% CI:0.19-0.70), but nobody has used trial data to analyze AESIs for these vaccines.
Critically, the Fraiman and Benn studies had a follow-up of only a few months after the second dose because Pfizer and Moderna, unfortunately, terminated their randomized trials a few months after receiving emergency use authorization. Of course, a longer-term benefit can provide a basis to tolerate negative or neutral short-term risk-benefit differences. However, that is unlikely since we know from observationalstudies that mRNA vaccine efficacy deteriorates a few months after the second dose.
There may also be long-term adverse reactions to the vaccine regarding which we do not yet know. Since the randomized trials ended early, we must look at observational data to answer that question. The publicly available data from the Vaccine Adverse Event Reporting System is of low quality, with both under- and over-reporting. The best observational data is from CDCs Vaccine Safety Datalink(VSD) and FDA’s Biologics and Effectiveness Safety System (BEST), but there have only been limited reports from these systems.
Fraiman and colleagues have produced the best evidence yet regarding the overall safety of the mRNA vaccines. The results are concerning. It is the responsibility of the manufacturers and FDA to ensure that benefits outweigh harms. They have failed to do so.
Uninformed Consent is an in depth look into the Covid 19 narrative, who’s controlling it and how it’s being used to inject an untested, new technology, into almost every person on the planet. This film explores our recent loss of human rights while weaving in the devastating impact of mandates and the deeply powerful story of one man’s loss. Hear the truth from doctors and scientists unafraid to stand up against Big Pharma and the Elite Class who profit from these mandates.
How is it that The HighWire’s reporting on Covid has been so far ahead? How did we know so much about the public health players, and the games they would play with lockdowns and vaccines? Because, they’ve done it all before. The HighWire presents “Vaxxed: From Cover-Up to Catastrophe,” the movie that exposes one of the biggest public health scandals of all time. They say ‘vaccines don’t cause autism,’ but they never told you this.
Europe is accelerating steps to roll back COVID restrictions as efforts to control the spread of the virus have failed and countries downgrade the threat posed by SARS-CoV-2.
Sweden and Switzerland joined Denmark, Norway, Finland, Ireland, The Netherlands, Italy, Lithuania, France and the UK in announcing they will lift COVID restrictions and open up their countries.
Top Israeli officials also announced this week they are abolishing the country’s “Green Pass” COVID vaccine passport for restaurants, hotels, gyms and theaters.
The policy update will take effect Feb. 6, Prime Minister Naftali Bennet’s government said, pending approval by a parliamentary committee. Israel’s proof-of-vaccination policy will remain in effect for events such as parties or weddings.
“To continue the green pass in the same way can create false assurances,” said Nadav Davidovitch, an epidemiologist and public health physician advising Prime Minister Naftali Bennet’s government. “It’s not reducing infections in closed spaces like theatres. It needs to be used mainly for high-risk places like hospitals, elderly care homes, or events when you are eating and singing and dancing.”
According to Politico, the Swedish Public Health Agency said it reassessed COVID as “not being socially critical” due to a better understanding of the Omicron variant, which is milder and associated with fewer hospitalizations.
“It’s time to open up Sweden,” said Prime Minister Magdalena Andersson. “The pandemic isn’t over, but it is moving into a new phase.”
The decision to open Sweden came a day after Switzerland, citing high immunity levels and the milder Omicron variant, announced it will abolish mandatory work-from-home and the quarantine rules beginning today.
The government also will lift health measures at the borders and tourists will no longer need to receive Swiss COVID certificates.
The Swiss government said it planned to phase out other restrictions after consulting with 26 cantons, employers, trade unions and parliamentary committees.
In two weeks, the government will determine the next steps to relax pandemic measures depending on the health situation, according to an official statement.
Options include a staggered exit strategy or an abrupt end to all COVID measures on Feb. 17.
Denmark to classify COVID as endemic disease
Just days before Sweden and Switzerland’s announcements, Denmark became the first country in the European Union to lift all COVID restrictions, reclassifying COVID as an endemic disease.
Danish Health Minister Magnus Heunicke on Feb. 1 wrote a letter to the parliament’s epidemiology committee stating COVID was no longer a “socially critical disease.”
Based on the recommendations of the committee, the government decided to scrap COVID restrictions.
The “rules will lapse when the illness will no longer be categorized as ‘socially critical’ on 1 February 2022,” Heunicke wrote.
The classification of a disease as “socially critical” gave the government authority to implement broad restrictive measures such as shutting businesses and making mask-wearing mandatory.
An endemic disease circulates freely but is recognized as posing less of a threat to societies.
“No one can know what will happen next December,” Heunicke told CNN on Monday. “But we promised the citizens of Denmark that we will only have restrictions if they are truly necessary and we’ll lift them as soon as we can. That’s what’s happening right now.”
When asked about vaccine mandates, Heunicke said:
“Luckily we don’t need that in Denmark … I’m really happy that we don’t need it because it’s a very troubling path to move that way.”
Søren Brostrøm, director-general of Denmark’s Health Authority agreed:
“I do not believe in imposed vaccine mandates. It’s a pharmaceutical intervention with possible side effects. You need as an authority, to recognize that. I think if you push too much, you will have a reaction — action generates reaction, especially with vaccines.”
Danish authorities will still recommend taking at-home tests when coming into contact with large groups of people and will make PCR tests available to the public. Travelers entering the country will still be tested upon entry.
Other European Companies drop COVID restrictions
Italy, France, Norway, Lithuania, England and Finland also relaxed restrictions, Bloomberg reported.
“We should discuss whether it’s time for us to take a different viewpoint and start unwinding restrictions even with a high number of infections,” Finnish Prime Minister Sanna Marin told reporters. “I hope that we can be rid of restrictions during February.”
At a meeting in Helsinki to discuss the pace of removing restrictions, the government decided to lift all limits on gatherings and ease restrictions on restaurants and bars on Feb. 14. Night clubs will remain closed until March 1. Cultural venues, events and sports will be free from restrictions.
Italian Prime Minister Mario Draghi’s administration met Wednesday to discuss how to curb restrictions. The government will initially focus on quarantine rules for children and plans to cut the 10-day isolation requirement down to five.
France on Wednesday ended mandatory work-from-home rules, eliminated requirements on face masks outdoors and lifted attendance restrictions at stadiums and theaters. However the country’s vaccine pass will remain in place until hospitals are able to function normally without canceling non-emergency procedures to make room for COVID patients in intensive care, Health Minister Olivier Veran said on Wednesday.
Asked whether France would require a second booster shot, Veran said it would depend on whether there were further mutations of the virus.
The Lithuanian government is dropping its requirement to present a vaccination certificate in public areas, such as restaurants and sporting events, and unvaccinated workers will no longer be required to undergo weekly testing.
Norway followed suit and lifted restrictions on private gatherings, bars and restaurants and will not require border testing.
England last week announced it was lifting its COVID restrictions. Beginning Jan. 27, face coverings were no longer required by law anywhere in England and the legal requirement for COVID passes to enter large venues and clubs were scrapped.
The government also dropped guidance for face-covering in classrooms, advice for people working from home and restrictions for nursing home visitors.
On Jan. 26, the Netherlands reopened restaurants, bars, museums and theaters as part of a broader easing of restrictions.
Lockdowns had little-to-no benefit on public health, analysis shows
Few studies, if any, have been carried out to determine whether vaccine passports and COVID restrictions actually lowered COVID cases, hospitalizations and deaths.
However, a recent analysis published by researchers at Johns Hopkins found COVID lockdown measures implemented in the U.S. and Europe had almost no effect on public health.
“We find little-to-no evidence that mandated lockdowns in Europe and the United States had a noticeable effect on COVID-19 mortality rates,” the researchers wrote.
The researchers also examined shelter-in-place orders, finding they reduced COVID mortality only by 2.9%.
Studies assessing only shelter-in-place orders found a mortality reduction of 5.1%, but when combined with other lockdown measures, shelter-in-place orders actually increased COVID mortality by 2.8%.
Researchers found limits on gatherings may have actually increased COVID mortality. They wrote:
“[Shelter-in-place orders] may isolate an infected person at home with his/her family where he/she risks infecting family members with a higher viral load, causing more severe illness. But often, lockdowns have limited people’s access to safe (outdoor) places such as beaches, parks and zoos, or included outdoor mask mandates or strict outdoor gathering restrictions, pushing people to meet at less safe (indoor) places.”
COVID lockdown measures also contributed to “reducing economic activity, rising unemployment, reducing schooling, causing political unrest, contributing to domestic violence and undermining liberal democracy,” the report said.