In 2019 Senator Richard Blumenthal grilled wireless industry representatives, who admitted the industry has done ZERO health & safety studies on 5G technology. Meanwhile, dozens of independent studies indicates that 5G is a risk to all biological life. Watch the video below.
During today’s Senate Commerce, Science, and Transportation Committee hearing on the future of 5G wireless technology and their impact on the American people and economy, U.S. Senator Richard Blumenthal (D-CT) raised concerns with the lack of any scientific research and data on the technology’s potential health risks.
Blumenthal blasted the Federal Communications Commission (FCC) and the Food and Drug Administration (FDA)—government agencies jointly-responsible for ensuring that cellphone technologies are safe to use—for failing to conduct any research into the safety of 5G technology, and instead, engaging in bureaucratic finger-pointing and deferring to industry.
In December 2018, Blumenthal and U.S. Representative Anna G. Eshoo (CA-18) sent a letter to FCC Commissioner Brendan Carr seeking answers regarding potential health risks posed by new 5G wireless technology. At today’s hearing, Blumenthal criticized Carr for failing to provide answers, and instead, just echoing, “the general statements of the FDA, which shares regulatory responsibility for cell phones with the FCC.” Blumenthal also decried the FDA’s statements as “pretty unsatisfactory.” A PDF of Carr’s complete response is available here.
We believe this crisis represents a world-changing opportunity to expose and transform antiquated ideologies that restrict health freedom. Germ theory is a scientifically bankrupt paradigm based in warfare models of pathogenic invasion. This theory has been leveraged as an instrument for geopolitical and social control – largely in the form of a vaccination agenda – to subdue the populace through coerced and forced bodily penetration and associated disability, mortality, and surveillance. As a result, conventional Western medicine functions as a sort of religion based on consensus assumptions and dogmatic medical monotheistic posturing. At its core, this approach is not salugenic or scientific and thus violates its stated ethical parameters around informed consent, beneficence, and an uncompromised evidence base.
We believe that citizens should be free to exercise their natural right to practice medicine as they see fit – in retention both of bodily sovereignty and civil liberties. To that end, we orient ourselves around the foundational premises that the body is inherently wise, that symptoms are meaningful, and that radical healing is eminently possible when we align with the earth and honor our place in the natural world.
While joining conservative host Hugh Hewitt on his radio show on Tuesday, Attorney General Bill Barr spoke out on the coronavirus lockdowns here in the United States, stating that the stay at home orders are beginning to do more damage than the virus itself.
Barr explained that the lockdown decision was initially a good move to slow the virus however he feels that it is starting to go for too long.
“These are unprecedented burdens on civil liberties right now. You know, the idea that you have to stay in your house is disturbingly close to house arrest,” Barr said. “I’m not saying it wasn’t justified. I’m not saying in some places it might still be justified. But it’s very onerous, as is shutting down your livelihood.”
The Attorney General continued by comparing the coronavirus shutdowns to chemotherapy treatments.
“Your first thing is to drive [the cancer] back to a more manageable state, and that’s what we’re doing and have done,” the attorney general stated. “The question is, you can’t just keep on feeding the patient chemotherapy and say ‘well, we’re killing the cancer,’ because we’re getting to the point where we’re killing the patient.”
Nearly 22 million people have applied for unemployment benefits in the past month, a rough estimate of the number of people that have either lost their jobs or been furloughed since states began implementing strict stay-at-home orders to slow the spread of the coronavirus. The Department of Labor reported the latest claims numbers on Thursday, and the number of jobs lost has likely continued to climb steeply since.
Protests have broken out across several states such as Michigan, North Carolina, and Ohio of residents demanding that state governors loosen stringent regulations that are forcing many businesses to stay closed.
The pain of many businesses has been compounded since the Paycheck Protection Program, a federal relief fund meant to float businesses through the pandemic, went dry last week. Democrats in Washington have delayed a fresh cash infusion to the program to secure more funding for state and local governments. A bill is expected to pass the Senate on Tuesday.
Nearly 805,000 people have tested positive for the coronavirus in the United States, and roughly 44,000 deaths have been attributed to the virus by Tuesday afternoon. New York, the state hardest hit by the pandemic, accounts for nearly half of total U.S. deaths with about 20,000.
A handful of states are preparing to relax emergency restriction in the coming days and will allow many people to begin working, albeit with some social distancing rules for the foreseeable future. Gov. Brian Kemp of Georgia is expected to be one of the first to begin opening his state, announcing on Monday that he would lift his stay-at-home order by the end of the week.
A federal investigation found CDC researchers not following protocol.
By Beth Mole
As the new coronavirus took root across America, the US Centers for Disease Control and Prevention sent states tainted test kits in early February that were themselves seeded with the virus, federal officials have confirmed.
The contamination made the tests uninterpretable, and—because testing is crucial for containment efforts—it lost the country invaluable time to get ahead of the advancing pandemic.
The CDC had been vague about what went wrong with the tests, initially only saying that “a problem in the manufacturing of one of the reagents” had led to the failure. Subsequent reporting suggested that the problem was with a negative control—that is, a part of the test meant to be free of any trace of the coronavirus as a critical reference for confirming that the test was working properly overall.
Now, according to investigation results reported by The New York Times, federal officials confirm that sloppy laboratory practices at two of three CDC labs involved in the tests’ creation led to contamination of the tests and their uninterpretable results.
“Just tragic”
Shortly after the problems became apparent in early February, the Food and Drug Administration sent Timothy Stenzel, chief of in vitro diagnostics and radiological health, to the CDC to investigate what was going wrong. According to the Times, he found a lack of coordination and inexperience in commercial manufacturing.
Problems that led to the contamination included researchers coming and going from labs working on the test kits without changing their coats and researchers sharing lab space to both assemble test components and handle samples containing the coronavirus.
The CDC said in a statement Saturday to the Times that the agency “did not manufacture its test consistent with its own protocol.” Though the CDC appeared reluctant to admit contamination was at the root of the problem, the Times noted that in a separate statement the CDC seemed to acknowledge such problems, saying the agency has since “implemented enhanced quality control to address the issue and will be assessing the issue moving forward.”
After the CDC first sent its test kit to states in early February, it took the agency around a month to fix the problem. By then, the virus had invaded many communities unimpeded, and any chance that the US had at containing its spread had virtually vanished. By mid-March, many states turned to mitigation efforts, such as social distancing, to try to blunt—rather than prevent—the life-threatening, healthcare-overwhelming effects of COVID-19.
“It was just tragic,” Scott Becker, executive director of the Association of Public Health Laboratories, told the Times. “All that time when we were sitting there waiting, I really felt like, here we were at one of the most critical junctures in public health history, and the biggest tool in our toolbox was missing.”
As of the morning of April 20, the US has confirmed more than 760,000 cases of COVID-19 and more than 40,700 deaths. The numbers are expected to be underestimates due to the slow and still limited amount of testing.
So, I had this hope that the next thing I posted here would be a grand explanation about my extended absence, all the weird stuff that’s happened over the past few years, my loss of faith in nutrition as a front-line approach to healing, and various other sundries I’ve been storing up in my brain-attic.
But then COVID-19 happened, and if that isn’t the biggest cosmic plan-changer that ever did plan-change, then I don’t know what is. So we’re gonna roll with it. And at the risk of writing something that’ll already be outdated by the time I hit publish (such is the nature of current events), I’m hoping this post will stay evergreen (or at least ever-chartreuse) by sheer virtue of its universal core theme: navigating conflicting, emotionally charged narratives in which objectivity behooves us but doesn’t come easy.
So LET US BEGIN.
In case you didn’t notice, the cyber-world (and its 3D counterpart, I assume, but we’re not allowed to venture there anymore) is currently a hot mess of Who and what do we believe? This is zero percent surprising. Official agencies have handled COVID-19 with the all grace of a three-legged elephant—waffling between the virus being under control/not under control/OMG millions dead/wait no 60,000/let’s pack the churches on Easter!/naw, lockdown-til-August/face masks do nothing/face masks do something, but healthcare workers need them more/FACE MASKS FOR EVERY FACE RIGHT NOW PLEASE AND THANK YOU/oh no a tiger got the ‘rona!; on and on. It’s dizzying. Maddening. The opposite of confidence-instilling. And as a very predictable result, guerrilla journalism has grown to fill the void left by those who’ve failed to tell us, with any believability, what’s going on.
Exercising our investigative rights is usually a good thing. You guys know me. I’m all about questioning established narratives and digging into the forces that crafted them. It’s literally my life. Good things happen when we flex our thinking muscle, and nothing we’re told should be immune to scrutiny.
But there’s a shadow side here, too—what I’ll henceforth refer to as “lopsided skepticism.” This is what happens when we question established narratives… but not the non-established ones. More specifically, when we go so hog wild ripping apart The Official Story that we somehow have no skepticism left over for all the new stuff we’re replacing it with.
And that, my friends, is exactly what’s happening right now.
I’ve been watching homegrown theories about COVID-19 spiral through various social platforms, born from a mix of data (sometimes) and theory (usually) and anecdote (always). They’re generally a pushback against the mainstream narrative about the coronavirus’s timeline, severity, concern-worthiness, fatality rate, treatment, infection breadth, classification guidelines, origin… round and round we go. Some theories are reasonable (“Has the virus been here longer than we think?”), some are untenable (“The ‘virus’ is actually radiation poisoning from 5G towers!”), and many more lie somewhere between.
Most importantly, they all have one thing in common: a tendency to embrace any and all supportive data without, well, making sure it’s true.
Y’all know what I’m talking about. Evidence we’d never give the time of day if it didn’t work in our favor. The “I remember reading somewhere…”, the “I have a friend who knows someone who…”, YouTube interviews that are impossible to fact-check (but please just trust this person’s top-secret info from an organization they can’t name without the Feds beating down their door), crowdsourced anecdotes, retracted papers, retweeted screenshots of Facebook comments from people whose names and profile pictures are blacked out, the whole shebang.
This stuff. Is. EVERYWHERE.
Unfortunately, throwing a bunch of really bad evidence together can create the illusion of a well-supported theory. And this is what’s happening, my dudes. This is what it’s come to. In our rabid quest to undermine the Powers That Be andfigure out what’s really going on, we’ve thrown quality control out the window and become that which we loathe: loyalists to narrative over data.
Case in point, let’s look at what might be the most popular COVID-19 theory circulating right now: that mortality stats are getting padded by assigning deaths to COVID-19 that are really from other causes—thereby making this whole thing seem worse than it actually is. Depending on the sub-theory, this might be due to financial incentives for hospitals (more COVID-19 patients = more $$$); a coordinated government hoax to trick people into relinquishing their sovereignty; a way to butter us up for mass ID microchipping; something something lizard people; and so on.
And from what I’ve seen—and by all means correct me if I’m missing something—this theory draws on the following claims:
The CDC has literally issued guidelines telling doctors and medical examiners to classify deaths as COVID-19 if they “presume” the patient has it—no test results needed.
CDC data shows a precipitous drop in pneumonia deaths right around the same time COVID-19 became a thing—suggesting pneumonia deaths have been getting reclassified as COVID-19 deaths, and creating the illusion of a pandemic.
People who die with coronavirus, but not from coronavirus, are getting counted as COVID-19 deaths—again inflating the body count.
Despite COVID-19 mortality skyrocketing, total mortality is staying the same (or even dropping)—suggesting a “cause of death” shuffle, if you will, and betraying the idea that we’re seeing additional deaths from a new disease. (Alternatively: “Only people with preexisting medical conditions are dying and they were gonna keel over any minute anyhow.”)
This theory would be pretty awful if it’s true. We’d have been got. Duped. Manipulated AF. But how solid is the evidence? Have we actually peeled this thing apart piece by piece before getting all ragey about the injustice of it all?
Oh, we haven’t? Well GUESS WHAT WE’RE GOING TO DO NOW?
Let the unpeeling commence.
Claim #1
1. First, the whole “CDC is telling people to report COVID-19 deaths without testing!” ordeal. The damning bits come from the CDC’s COVID-19 reporting guide (PDF), which gives permission to use COVID-19 on a death certificate if it’s “suspected or likely” and “‘probable’ or ‘presumed’”:
And also says it’s okay to report COVID-19 without testing confirmation:
The point of contention here, which has sparked something of an outrage in important places such as Twitter, is that these guidelines allow a level of guesswork that could mess things up real bad. Especially if there’s already some sort of incentive to bend data in the direction of more coronavirus deaths. What if people assign COVID-19 willy nilly to anyone who has a cough or fever? Or who had a poorly-timed bout of allergies? Where does the line get drawn? For sure, “probable,” “presumed,” “suspected,” and “likely” aren’t very reassuring words when it comes to a disease we’ve shut down the whole globe to contain.
But is this actually conspiracy worthy? And, in a clinical setting, with actual doctors doing doctor things rather than us internet-dwelling oafs imagining how it all might go, would these guidelines really lead to a significant over-reporting of COVID-19 deaths?
For starters, let’s look more closely at that CDC reporting guide. Although it does say COVID-19 deaths can be assigned without a positive test result, it also emphasizes the importance of drawing from all available evidence in order to make an informed judgment:
And medical examiners are broadly allowed to list “causes that are suspected,” and to “use words such as ‘probable’ or ‘presumed’”—again, for any death-cause:
And here we see the CDC’s Instructions for Completing the Cause-of-Death Section of the Death Certificate telling us again that a condition can be listed as “probable” even if there isn’t a definitive diagnosis (and also the words YOUR and OPINION written in CAPS because the CDC successfully learned how to yell on the internet; good job, CDC):
*I know it’s tiny; click for bigger
Are you sick of this yet? Guess what? Alzheimer’s deaths can get the same code whether the disease is confirmed or “probable”:
Oh hey, remember 83 seconds ago when we were so mad that COVID-19 deaths could be listed as “probable” or “presumed”? Because it seemed like some unique-to-coronavirus word twist intended to help pad the death stats? REMEMBER?
No. Just no. This same language is consistent through all the cause of death guidelines, no matter the killer in question. It’s been that way for years. And COVID-19 is even lucky enough to get separate codes for “probable” versus “confirmed” cases, which is more than we can say for some other diseases. (And to boot, some places were already seeing COVID-19 mortality explode before reporting the “probable” deaths at all.) Heck, the guidelines for coronavirus deaths are far more straightforward than the maze-like estimation formula the CDC takes for flu mortality.
In short—and please make me eat my words if I’ve overlooked something important here—this really isn’t outrage-worthy. Certifying any form of death is an imperfect, partly subjective process, and concessions for that reality are baked into all sorts of official guidelines. If overzealous COVIDing is happening (and you’re welcome to investigate any theory-offshoots that it is), it’s not because the CDC told death certifiers to cook the books.
Claim #2
2. As for pneumonia deaths getting classified as COVID-19 deaths? This graph of CDC data has been making the rounds as evidence that something very shady, very shady indeed, is going on. As you can see, around week 10 of this year (starting March 2nd), pneumonia mortality told its wife it loved her and then jumped off a cliff:
If we’re already primed to think the COVID-19 numbers are being doctored, we might take this graph at face value and add it to our stash of outrage fodder. But that would not be smart, friends. Face value is where critical thinking goes to die. And so, in the spirit of questioning literally everything, we must ask: could anything else explain what we’re seeing?
As a matter of fact, yes! So much yes! We only have to venture as far as the CDC’s Provisional Death Counts for Coronavirus Disease (COVID-19) page to see what’s up. Go take a look. Especially the “Delays in reporting” section. Thar be some gold.
Basically, the CDC’s death-certificate-processing system is a slow, laborious beast that ensures any recent mortality data is always incomplete. They give a decent rundown of how death certificates get handled from start to finish:
Provisional counts of deaths are underestimated relative to final counts. This is due to the many steps involved in reporting death certificate data. When a death occurs, a certifier (e.g. physician, medical examiner or coroner) will complete the death certificate with the underlying cause of death and any contributing causes of death. In some cases, laboratory tests or autopsy results may be required to determine the cause of death. Completed death certificate are sent to the state vital records office and then to NCHS for cause of death coding.
And here we have a special shoutout to our favorite infectious diseases, noting that pneumonia, flu, and COVID-19 certificates take extra long to trickle into the data pool due to manual coding (emphases mine):
At NCHS, about 80% of deaths are automatically processed and coded within seconds, but 20% of deaths need to manually coded, or coded by a person. Deaths involving certain conditions such as influenza and pneumonia are more likely to require manual codingthan other causes of death. Furthermore, all deaths with COVID-19 are manually coded. Death certificates are typically manually coded within 7 days of receipt, although the coding delay can grow if there is a large increase in the number of deaths. As a result, underestimation of the number of deaths may be greater for certain causes of death than others.
Zooming in even further, the CDC gives some stats conveying just how incomplete their recent data is, and boy howdy is it a sorry sight. At any given moment, data from two weeks ago is likely to be barely over a quarter complete, while data from eight weeks ago is still less than three-quarters complete:
Previous analyses of provisional data completeness from 2015 suggested that mortality data is approximately 27% complete within 2 weeks, 54% complete within 4 weeks, and at least 75% complete within 8 weeks of when the death occurred.Pneumonia deaths are 26% complete within 2 weeks, 52% complete within 4 weeks, and 72% complete within 8 weeks (unpublished). Data timeliness has improved in recent years, and current timeliness is likely higher than published rates.
The CDC even slaps this little disclaimer after each table of COVID-19, pneumonia, and flu death counts:
Once again, with feeling: CDC mortality figures are initially very incomplete, low-balled-as-all-get-out, and retroactively fill in over time. Which means a weird pneumonia death-drop will show up any time we check the most recent data, COVID or No-vid.
To illustrate, Joseph Dunn graphed the CDC’s pneumonia data as it appeared on the same mid-March week of each year since 2013. Behold:
Look at all them swan dives!
And data scientist Tyler Morgan even went to the trouble of graphing the data from every weekly CDC pneumonia report published in the last decade, to show how the lines shift as data gets back-filled. Click here or on the image below for the really cool animation (it’s weirdly beautiful and absolutely worth the 30 seconds of your life):
In other words, there’s nothing anomalous at all about 2020’s pneumonia trends. Nothing. The popular graph up top is a meaningless piece of hooey and it’s sad that it went viral.
Note: there’s an issue here I’m cognizant of, but intentionally not touching on yet, which is that some people believe the CDC (and any other government organization) literally makes up data from thin air, thus rendering all of the above irrelevant. This level of conspiracy is beyond the scope of this post, but I may try to address it at some point later on. Not from a data angle, but from a psychological one.
Claim #3
3. Here we have the wildly popular claim that people are dying with COVID-19, not really from COVID-19. At least, not in the numbers we’re being told. It’s basically a steroided-up version of Claim #1—just with more trickery and plot-thickness and finger-tenting.
The evidence for this one is a lot harder to fact-check, because there are actually no facts to check. Its trueness rests on us believing that doctors and death-certifiers are being marionetted by evil forces and/or just plumb don’t know what they’re doing.
The closest thing we’ve got to “evidence” are citationless social media statements like the above, which we’re expected to trust because LOOK AT ALL THOSE RETWEETS!, a few well-publicized examples of allegedly mis-assigned COVID-19 deaths, and Youtube interviews with people who are pretty sure they know what’s going on. Like this one, featuring Dr. Annie Bukacek, with nearly 750,000 views at the time of writing.
Apparently, she knows her stuff. And the stuff she knows is that the coronavirus figures are being manipulated!
Hmmm…
Hmmmmmm…
Hmmmmmmmmm.
Serious question: how many of us bothered to look Dr. Bukacek up before thrusting her atop a pedestal of trustworthiness? And sharing her video far across the lands? And assuming she’s an impartial commentator on the whole situation (her praiseful introducer was literally her pastor)? Should we really put faith in someone we didn’t even know existed ten seconds ago just because 1) they’re telling us what we want to hear and 2) an internet headline made them sound prestigious?
By the way, to state the obvious, this is me intentionally and very shamelessly cherry-picking to make a point. Not all of her reviews are bad. Nor do the existing ones necessarily prove she isn’t credible. And if we wanted to be truly fair, we could prod deeper and ask whether she might be getting bad-review-bombed due to her vocal pro-life activism or religious affiliation or anti-vaccine stance (she’s definitely got some haterz). There’s a lot of sticky tricky gray-zone business in evaluating reputation, which is why—whenever possible—we should investigate a person’s claims rather than their character.
But the issue here is that with Dr. Bukacek, we can’t “investigate her claims” without installing cameras into every death certifier’s brain and watching what unfolds within their basal ganglias. So we’re left with only her word. And one person’s word is not useful data. Even if it’s the best of persons and the best of words.
Now, to play devil’s advocate with my own arguments here, there’s another popular video—this one featuring Coronavirus Response Coordinator Deborah Birx—that seems more genuinely suspect. I saved this one for last because it might actually have some merit. In it, Dr. Birx talks about the USA’s “very liberal approach to mortality” and outright states that people who die with COVID-19 are counted as COVID-19 deaths:
Transcript: There are other countries that if you had a preexisting condition, and let’s say the virus caused you to go to the ICU and then have a heart or kidney problem, some countries are recording that as a heart issue or a kidney issue and not a COVID-19 death. Right now we’re still recording it and we’ll—I mean the great thing about having forms that come in and a form that has the ability to mark it as COVID-19 infection, the intent is right now that those—if someone dies with COVID-19 we are counting that [as a COVID-19 death].
It’s not surprising this clip went gangbusters! It seems like a deal-clinching A-ha for anyone who suspected COVID-19 was getting slapped onto every death possible.
However, here and always, context matters. After all, this segment was carefully cropped from a much longer coronavirus briefing from April 7th. And if we listen to the full segment—the audience question that came before this clip, and the follow-up question that came after it, and the follow-up answer Dr. Birx gave, and the addendum answer Dr. Anthony Fauci gave—we can better orient ourselves in the conversation that was happening.
Go have a listen. The relevant stuff starts at the 1:39:07 mark:
Could it be that Dr. Birx thought the question-asker was wondering if lack of testing might cause under-reporting, and tried to reassure her by explaining that the current COVID hotspots are flush with tests? And that people with “heart or kidney problems” wouldn’t be reported as dying from those things if they’d ended up in the ICU from coronavirus? (Especially given that COVID-19 itself can cause cardiac injury and kidney damage?)
It sounds to me like the thrust of the asker’s question—which was more along the lines of “Are we sure we’re not over-counting deaths?!”—went over the heads of the task force, and they addressed a different issue than the one she was trying to get at.
But I can’t read minds. And I can’t prove that it’s not all just political doublespeak and of course they understood the question. And I think there’s far too little information in this video alone to assess it from a “scam vs. not-scam” angle. And most importantly, in the absence of actual mortality data that could clue us in to potential over-reporting, I doubt analyzing this thing to smithereens can bring us any closer to the truth.
But, you be the judge. And speaking of mortality data…
Claim #4
4. Lastly and not leastly: the claim that COVID-19 isn’t actually causing excess mortality; we’re just reshuffling death causes to stack up higher for COVID-19 and lower for everything else. Boom, insta-pandemic!
First, a note. This is a Very Important claim. It’s the supreme ruler of all the claims that came before it and perhaps all those incipient ones that will come after. It has executive power and a VIP card for entry into the most highly guarded chambers of our brains. This is because, unlike causes of death, actual body counts can’t be fudged. This is the one true test. If COVID-19 really is taking lives en masse above and beyond what we’d expect from normal death trends, total mortality is where it’ll show up. If it’s not, then our game of death-code musical chairs will be revealed for the con that it is.
Again: Very Important claim. This is the crux of it, my dear readers.
Fortunately, there’s an easy way to test this claim: looking at total mortality trends in areas that COVID-19 has purportedly ravaged, and comparing that to historical mortality in the same location. An absence of anomalous death spikes—taking into account, of course, delays in processing death certificates and the lag time between infection and dying—would suggest we’re over-reporting COVID-19. And if excess mortality does appear, then we either have to concede that COVID-19 isn’t a nothingburger after all, or propose that some other ghastly, unnamed entity is stealing lives very coincidentally at the same time we have a made-up pandemic.
*Keep in mind, too, that our current near-global quarantine should slash deaths from accidents and certain crimes and infectious disease—and thus “normal” mortality rates for right now would likely be lower than for previous years.
So let’s dig into this. The “COVID-19 is overblown” theory asserts that total mortality isn’t doing anything unusual. At least not significantly so. No more than a bad flu year, let’s say. And depending on the source, we may be furnished with graphs that seem to demonstrate this truth to our hungry, data-seeking eyes, such as the following for England and Wales:
There’s one very big problem here. Check the dates.
Almost universally, the “See, it’s nothing!” graphs use data from mid to late March, when COVID-19 was just starting to pick up steam in the areas it’s most recently terrorized. And in March, there really weren’t massive mortality spikes, except perhaps for Italy. Nothing to see here, folks was true. And no one in the infectious disease world was claiming otherwise. In March, the rumblings of upcoming mortality explosions was what people were getting worried about, not the numbers as they then stood. The whole deal with “exponential growth” is that it’s—wait for it—exponential. This is how we went from 0 reported COVID-19 deaths in the USA on February 15th, 65 deaths one month later, and 30,000 deaths yet another month later.
So let’s see what happens when we look, instead, at more recent data from countries with known COVID-19 outbreaks. (This site is a great starting resource for raw mortality data and some visuals.)
First, here’s what’s up with England and Wales now (source):
And another depiction suggesting COVID-19 deaths may be under-reported (data source and image source):
A big chunk o’ Europe getting excess-mortalitied (source):
New York City, graphed by the New York Times (article here; viewable with free subscription) (NOTE: this data is almost two weeks outdated and the the April deaths are now many magnitudes higher):
We could do this all day, but you get the point.
Here’s the deal, folks. People. Are. Dying. The mortality trends for COVID-19-affected areas look like what happens when you’re trying to draw a straight line and then sneeze. This is not normal. This is not how things “should” look. We can argue all we want about how accurate the COVID-19-specific data is—and indeed, there’s plenty to argue about— but total mortality doesn’t lie. This is real.
Final Thoughts
By all means, the above peel-apart is far from complete. I’m sure there are more viral videos we could assess, more statistics to double-check, more anomalies to ponder. The point isn’t to reach a final conclusion here—just to demonstrate the process. The level of detail that must go into investigating a theory before we let ourselves fully entertain it. And if that process seems exhausting, excessive, excruciatingly nit-picky, too time consuming—well, it’s the price of admission for calling ourselves “informed.” Anything less and we’re operating on faith. Which is okay, if that’s our goal. But we must call it what it is.
Now maybe you’re thinking, “Okay, the ‘COVID-19 deaths are getting padded’ theory didn’t really hold up. But what about G5 radiation causing virus symptoms? What about mandatory vaccine agendas getting pushed on the world? What about COVID-19 being a bioweapon? What about what about what about?”
To which I say, Yes! Great! What about them indeed! Put on your best-tailored thinking cap and go find out. Marinate in all the data you can find. Watch out for claims that seem sciencey but trace back to a 4chan post. Be mindful of the universal human tendency to filter out things we disagree with and embrace any evidence that we like. Dig in, first and foremost, with the goal of proving yourself wrong. If you can’t, then perhaps there’s something there.
Of course, I realize the type of deep-dive we did in this post isn’t always possible, and not everyone can sit at home all day opening so many browser tabs that their MacBook freezes with a “System Has Run Run Out of Application Memory” error (anyone else? No? Just me?). Sometimes we need shortcuts. So for anyone who really wants to do the work, to prioritize truth-seeking over ideology, to stay oriented in reality, to let go of false narratives, but who doesn’t have infinite time to do so: here are some questions to ask whenever a new or alternative theory presents itself. Especially a theory we find ourselves enamored with. None of these questions can substitute for ruthlessly investigating, but they can help us stay grounded in situations where our minds easily lead us astray.
Am I claiming to see through the media’s fear-mongering, but falling prey to conspiracy fear-mongering instead?
Am I being pressured to accept this theory in order to be “woke” or “not sheeple”?
Have I read the full context of this quote, clip, or screenshot before assuming I know what it means?
Does the group promoting this theory invite questions and critiques? Or does it flippantly dismiss those things and/or attack its doubters?
If this same form of evidence (Youtube interview, social media comment, etc.) was used to support the “other side” instead of mine, would I still consider it trustworthy?
Am I taking time to research counter-arguments to these ideas, even when I want them to be true?
Am I looking for good vs. evil narratives as a distraction from my immediate reality? Is getting worked up about hypothetical injustice easier than being present with what is?
Am I embracing this theory as a way to feel like I have control—by naming an enemy in a situation where I’m otherwise helpless?
Does seeing myself as a “good guy” on the side of “truth” or “justice” make me feel validated, empowered, and important?
It’s easy to trick ourselves into thinking we’re being Good Skeptics when we’ve really only lifted one veil of many. There’s nothing “woke” about rejecting the official story while gullibly swallowing its alternatives.
Rather, waking up means waking up to ourselves. It’s recognizing that the battle of good and evil we project onto the world is playing out daily within ourselves. It’s committing to seeing “what is,” instead of stories about “what is.” It’s spreading our skepticism evenly across the info-scape instead of saving it for the things we already distrust.
So here it is, you guys. This is me groveling at the collective feet of the internet, with one thing to say: to anyone—everyone—listening, we need to reflect on how we’re processing the claims we hear. If we’re going to question official narratives, we need to question alternative narratives with the same degree of rigor. There’s no use retiring our sheeplehood from the mainstream only to rejoin the herd on a different pasture.
These are quarterly meetings held every 3 months, as required by law, but seldom, if ever, publicized or reported on by the corporate “mainstream” media.
Health Impact News might be the only place where these quarterly meetings are reported, and you can review past reports here. We have been accused of publishing “Fake News” when we publish these reports, but all of the information is available to the public and posted on the Federal Government’s websites.
The Big Tech companies that control so much of the Internet’s traffic, work hard to suppress this information. If you visit one of Health Impact News‘ Facebook Pages, for example, you are likely to see this notice inserted to the top of our page:
The March 6th meeting by the Advisory Commission on Childhood Vaccines included a report from the Department of Justice (DOJ) on cases settled for vaccine injuries and deaths as mandated by the National Vaccine Injury Compensation Program (NVICP).
The NVICP was started as a result of a law passed in 1986 that gave pharmaceutical companies legal immunity from being sued due to injuries and deaths resulting from vaccines.
If you or a family member is injured or dies from vaccines, you must sue the federal government in this special vaccine court. Many cases are litigated for years before a settlement is reached.
The March, 2020 DOJ report states that 288 petitions were filed during the 3-month time period between 11/16/19 – 2/15/20, with 181 cases being adjudicated and 146 cases compensated.
The March, 2020 DOJ report lists 74 of these settlements for vaccine injuries and deaths, and 60 of those were for damages caused by the flu vaccine. Read more…
Editor’s Note: This is a fine overview and summary of the film about the origins of the Wuhan virus.
By Jo-Est B. Tan
Part 1. The Story of The Seafood Market
The Wuhan Health Commission released an internal notice on December 30, 2019 saying, “There has been a continuous occurrence of pneumonia cases of unknown cause at Huanan Seafood Market”
Shortly afterward, the Wuhan Health Commission issued a public notice saying that new pneumonia cases were related to the seafood market, but did not transmit virus from human to human.
“Some medical institutions found a link between the pneumonia cases and the Huanan Seafood Market” but that “there was no evidence of ‘obvious human to human transmission’ and no infection among medical personnel.”
So on January 1, 2020, the Huanan Seafood market posted a notice of closure, and had a thorough clean up. Guan Yi, a Hong Kong expert mentioned that it was like they were trying to cover up a crime scene. Officials in Wuhan said that most of the pneumonia cases have had a history in the Huanan Seafood.
On January 26, 2020, the Institute of Virology of China, CDC said that 33 of the 585 environmental samples from Wuhan market had the novel coronavirus nucleic acid, and added that the virus came from wild animals in the market.
On January 24, The Lancet produced an article called Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China that suggested the virus might not have originated from the market.
The first author of the paper was Huang Chaolin, the Deputy Director of Jin Yin-tan Hospital, and this facility was the first to treat patients with the unknown pneumonia in Wuhan.
Dr. Sean Lin, former Lab Director of the Viral Disease Branch, Walter Reed Army Institute of Research said the symptom onset of the first patient was on December 1, 2019, and had no relation to the Huanan Seafood Market, and no epidemiological link was found between the first patient and later cases.
On December 10, 2019, there were 3 more cases, and 2 of the 3 cases had no relation to the Huanan Seafood Market.
Since December 15, 2019, a cluster of cases with a history of seafood market exposure have been reported. Soon after the December 10, 2019 analysis of 3 patients, there were 14 of 41 patients studied that were found to not have been to the Huanan Seafood Market.
Judy A. Mikovits, Ph.D., a molecular biologist and former Director of Lab of Antiviral Mechanism NCI, pointed out that a Lancet article said that patient zero was did not even go to the seafood market, and that there are no bats at the market or anywhere close. However, a high similarity of SARS CoV-2 nucleotide sequences were found with bat-related viruses.
But reports from NBC and Fox News have stated that bats are a likely source of the Coronavirus COVID-19 pandemic.
On Janaury 29, The Lancet said 50 of the 99 cases from Jin Yan-Tan, were unrelated to the market.
The New England Journal added that the 45 cases confirmed before January 1st have not been to the market. This information came from two authors who are doctors and medical experts from China.
Daniel Lucy, an epidemiologist from the University of Georgetown said that if the Lancet paper was accurate, the first case would have been infected as early as November 2019 because due to the incubation period of the virus.
This can only mean that the virus was spreading in different areas in Wuhan before the reports suggested that the pneumonia cases had a history of exposure to the seafood market that reportedly started on December 15.
The first panel of experts from the National Health Commission arrived in Wuhan on December 31, 2019. After investigating cases in Jin Yin-Tan hospital, they said that the initial criteria for a confirmed case are fever, history to the seafood market, and whole-genomer sequencing.
The second group of experts that consisted of Zhong Nanshan arrived on January 18th and revised the criteria. They questioned why exposure to the seafood market would be a criterion when one third of the cases were unrelated to that area.
Dr. Lin pointed out the existence of a clear outside source of the infection and possible malfeasance involved in the Chinese information that the CPP is trying to cover up.
“It can go a long way to covering up the actual source by imposing a false place and you’re not looking at the actual victims, then you’re only allowed to find your keys under the light post,” said Mikovits.
Asian Affairs Experts Columnist Gordon Chang thinks the reports of deaths and cases by China are highly ‘suspicious’.
“Beijing for six weeks, in December, in January, suppressed information of the epidemic and then when they officially acknowledged it on January 20, they then started a campaign of suppression of information.
“We know that because the central leading group that was announced on January 26 has a nine person roster, and it’s very heavy with propaganda officials.
“The vice chairman of the group is the Communist Party’s propaganda czar. It appears that the Party’s main goal here is suppression of information, controlling the narrative. That’s more important to them than actually ending the epidemic,” he said.
Part 2 The Mysterious Gene Sequence
China released the full genome sequence of the Wuhan novel coronavirus on January 10, and virologists worldwide started analyzing it.
On February 3, a paper by Zhang Yongzhen from the National Institute of Communicable Disease Control and Prevention and his team, along with the School of Public Health of Fudan University was published by Nature which claimed that the Wuhan coronavirus is closely related to CoVZC45 and CoVZXC21, which are viruses sampled from bats in Zhoushan by the People’s Liberation Army.
The Wuhan coronavirus has an 89.1% nucleotide similarity to the CoVZC45 and exhibits 100% amino acid similarity in the NSP7and E proteins.
Other scientists then used Blast, a program developed by the National Institute of Health and the National Center for Biotechnology Information to compare the viral sequence based on the data released by Chinese authorities on January 12, and the results match with Zhang’s findings.
Scientist Lu Roujian from Chinese Center for Disease Control and Prevention published a paper in The Lancet on January 30 saying the Wuhan Virus has an 88% similarity to two bat-derived SARS-like coronaviruses collected in Zhoushan, Zhejiang Province.
Additionally, a 2018 paper says that scientists from the Research Institute for Medicine of Nanjing Command have confirmed that there are many SARS-like coronavirus in Zhoushan City which are referred to as Zhoushan virus.
Philipp explains that the Wuhan coronavirus is highly similar to a bat SARS-like coronavirus discovered by the Nanjing Military Research Institute with 100% amino acid similarity in NSP7 and the envelope protein (e protein).
With that information out, Dr. Lin thinks that this might have been created somewhere, just not in a natural environment.
“Hard to see a protein is 100% identical when the virus jumps species. That’s suggesting maybe the virus could be generated with a reverse engineer process.”
Mikovits says the similarity “can’t possibly be a natural mutation.”
“It almost certainly is a recombination event that was laboratory driven,” she said.
Philipp discovered that on January 21, “researchers from the Institute Pasteur Shangai Chinese Academy of Sciences published a paper in Science China Life Sciences suggests that a key part of S protein of Wuhan virus has high homology with the SARS virus.”
The S proteins allow the virus to enter human cells.
“The S proteins are like little mushrooms attached to the surface of the virus. These are also known as spine proteins or spike proteins and are an important tool for the coronavirus to invade human cells.
“The S protein acts as a key which can unlock the lock on the surface of the cell and then invade the cell to propagate and destroy it.”
Dr. Lin says this is the reason for multiorgan failure.
“That’s probably one of the important reasons contributing to multiorgan failure. They can spread out in the human body much faster.”
Mikovits says the virus couldn’t possibly enter human cells without the S protein.
“That’s the lock and key. That’s going to be what drives it right through human cells.
“So now you’re allowing that access to human tissues because the spike proteins of the natural evolutionary strains don’t infect human cells at all.
“And clearly if that spike protein from SARS weren’t on the new COVID-19 or SARS2, it wouldn’t be able to enter human cells.”
This only shows that the virus was modified in a laboratory,
“This is evidence that it couldn’t’ go through the seafood market because how did you get that spike protein off the original SARS from bats or any other way.”
“It’s lab-derived,” she added.
The Shanghai P3 laboratory, which first shared the Wuhan coronavirus genome, was then ordered by authorities to stop operating on February 28. Professor Zhang Yongzhen and his team worked on this laboratory.
A February 26 report on Caixin, a media company associated with the CPP, says Zhang and his team isolated and completed the genome sequence of the unknown virus on January 5.
On the same day, the Shanghai Public Health Clinical Center this to the National Health Commission, and recommended prevention measures.
No response was given as of January 11, so the team publicized the sequence on virological.org, which is the first worldwide.
On January 1, the Hubei Health Committee ordered genome sequencing organizations saying “Existing virus samples must be destroyed. Information about the samples, related papers and related data are all prohibited from release”
The Chinese science community was basically told to keep quiet.
Chang thinks that the CPP is just plain dangerous.
“It’s the response to this virus is extremely troubling. It ignored it for six weeks. It allowed it to spread around China. This is dangerous, irresponsible behavior.”
Former US Air Force brigadier general Robert S. Spalding says that China is responsible for every COVID-19 case.
“Every person that it harms is directly attributable to the Chinese Communist Party.”
Part 3 The Discoveries of Dr. Shi Zhengli
Dr. Shi Zhengli, virologist from the Wuhan Institute of Virology, has been studying bats and coronaviruses for many years and was the first to locate the key to how cross-species transmission can happen that would infect humans.
Zhengli has been researching about coronavirus since the 2003 outbreak. Since 2010, Zhengli and her team have been studying how coronaviruses can be transmitted to humans.
In 2010, Zhengli and her team finally published a paper showing how they discovered “the passageway for coronaviruses to enter human bodies.”
Another paper published by the same team in 2013 showed that they were able to successfully isolate 3 viruses from bats, and one of those had an S protein that integrated with human ACE-2 receptors, which only suggested that “direct human infection of SARS-like viruses to humans without the need for an intermediate host.”
Furthermore, in a 2015 paper, her team discussed a synthetic, and self-replicating Chimeric virus. This virus basically had the ability to allow for cross-species infection. Animals trials were also done on mice and subjects had lung damage that had no cure.
“Zhengli’s successful splicing of the SARS virus was a key to open the door to the cross-species transmission.”
Zhengli then mentioned she wanted experiments on primates.
“Her move to research on primates suggest this was to more closely simulate the infection of humans, with this new synthetic virus.”
This had the academic community concerned.
Simon Wain-Hobson of the Pasteur Institute in France told Nature, “If the new virus escaped, nobody could project the trajectory.”
Mikovits thinks that this is just evidence that the virus was made in a laboratory.
“Her work proves the hypothesis that it could not possibly have been generated in a natural, zoonotic transmission but had to come from a hospital setting, the laboratory setting, the bio safety level 4 Wuhan research facility.”
On November 14, 2018, Zhengli gave a presentation called “Studies on Bat Coronavirus and its cross-species infection”. The Shanghai Jiao Tong University has since deleted reports of the study on their website.
Chang thinks that since China is blaming the US for the virus, the latter should just lay out the facts.
“The US needs to defend itself because China is propagating this narrative that we [US] spread the coronavirus to China.”
“The US needs to just come out with the facts about how China took coronavirus samples from Canada and the US, they sent them to Wuhan.”
Part 4 The Secret of the Wuhan P4 Laboratory
On February 3, Zhengli published a paper on Nature on February 3 saying the virus was of “probable bat origin”, and used the same key as SARS to infiltrate human bodies.
Zhengli added that the 2019-nCov genome sequence was 96.2% consistent with a bat coronavirus originating in Yunnan, China called RaTG13, suggesting the Wuhan virus comes from a natural source.
But it drew skepticism, as the outbreak started in Wuhan, the place where the P4 laboratory is located that has various similar viruses and might leakage might have happened. But the government decided to blame the seafood market, which doesn’t even sell bats.
Chinese authorities prevented international experts from joining the investigation and attacked doctors such as Li Wenliang who disclosed the outbreak for spreading rumors.
The big question is why would the CCP censor information if the virus did actually come from a natural source?
Chang says that the alleged origin of the virus is peculiar to say the least.
“Almost every disease that starts in China begins in Guangdong Province that surrounds Hong Kong in the south, but Wuhan is in the central portion of the country, and so this was extremely unusual.”
The Lab Origin theory can’t even be considered a conspiracy since no there is no definitive answer regarding the origin of the virus.
“It’s not a conspiracy theory to think that the coronavirus came from the Wuhan lab. And until we know [the truth], the theory about the lab origin is certainly something that we should consider.”
On January 2, an email from the Director-General from the institute said, “Notice regarding the strict prohibition of disclosure of any information related to the Wuhan unknown pneumonia. “
“National Health Commission clearly mandates that all detection, empirical data, results, and conclusions related to this outbreak cannot be published on self-media or social media, nor disclosed to any media (including state media) or collaborative organizations (including any technical services companies”
On January 21, ”a new drug, “Remdesivir” provided to China by the US for Wuhan Coronavirus treatment was patented by the Wuhan Institute of Virology”
During the month of February, a lot of things happened regarding the P4 laboratory.
On February 3, Dr. Wu Xiaohua blew the whistle using his real name that Shi Zhengli’s haphazard laboratory management may have led the Wuhan virus to leak from the lab.
On February 4, Chairman of Duoyi, Xu Bo, blew the whistle using his real name that the by Wuhan Institute of Virology was suspected of manufacturing and leaking the Wuhan virus
On February 7, “Top Biochemical Weapon Expert” of the People’s Liberation Army, Chen Wei, officially assumed control over the Wuhan Institute of Virology’s P4 laboratory.
On February 14, Xi Jinping called for the inclusion of biosecurity into China’s national security framework, and to accelerate the introduction of a biosecurity law.
On February 15, the Institute refuted widely spread rumors on Chinese social media that female graduate Huang Yanling was patient zero, and had perished. However, Huang’s photo, CV, and thesis were all removed from the institute’s website, leaving only her name.
On February 17, Institute researcher Chen Quanjiao, blew the whistle using her real name that Director-General of the Institute, Wang Yanyi, was suspected of leaking the virus.
In addition, Dr. Francis Boyle, famous for drafting the Biological Weapons Anti-Terrorism Act of 1989, said, “The novel coronavirus we’re facing here is an offensive biological warfare weapon.”
In 1999, the People’s Liberation Army published a book called “Unrestricted Warfare” discussing how weaker nations can fight against stronger nations in the context of modern warfare.
Author Qiao Liang wrote “After the first Taiwan Strait crisis, we realized that if Chinese and American military fought head on, we are at a disadvantage. Therefore we need a new strategy to help our military tilt the balance of power”
The Federation of American Scientists expressed concern saying that the CCP has advanced chemical warfare projects, including research, development, manufacturing, and weaponizing capabilities.
Spalding thinks China wants to be the best in biological weapons.
“I believe they have them. I think they want to be the most advanced nation on earth when it comes to biological weapons.”
Anthony Shaffer, former CIA trained officer says that China has some big plans.
“There’s a lot of concern about what China’s ambitions are regarding long term global domination.
“Their military doctrines indicated that they intend to be the dominant political and military force to Pacific Rim”
Chang says that the US should start defending itself since China has declared ‘war’,
“Last May, the communist party, through People’s Daily, carried a piece which said there was a “people’s war” against the United States. There is a war. China told us there’s one.”
Part 5 Facing The Pandemic
The virus has spread to 190 countries. Europe is now the center of the outbreak, and the US has called a state of national emergency.
Spalding emphasizes that China has a strong influence on many organizations, including the World Health Organization.
“All you have to do is look at the photo of Tedros (Adhanom, Director-General of WHO) and Xi (Jin Ping, Chinese president) shaking hands. It really is indicative of how China controls many of these international institutions.”
“You can see that the WHO is essentially following Chinese communist party’s guidelines.”
Chang similarly acknowledges how China is willing to go the extra mile to conceal essential information.
“From the very beginning of the coronavirus outbreak, the communist party has done its best to prevent the CDC and others from studying the origin of the disease.”
Mikovits says that the real fight is not against the virus, but against the CPP.
“The biggest issue is fighting a system that is determined to cover up and persecute anyone who reveals the truth behind.”
Chang thinks the same.
“Every country has diseases, but in China they become national emergencies and global emergencies because the real disease here is communism.”
Philipp also added that the scientists who suggested the lab theory declined to be interviewed and avoided questions regarding the virus.
Shaffer thinks the media such as those In the US have also been influenced by China because they wouldn’t discuss subjects that are sensitive to China being responsible for the deaths of thousands.
“In this case there is a lot of things not being said.”
Spalding says that this is because those media companies make a lot of money from China, and if they go against the country’s wishes, then they would suffer great consequences.
“Chinese communist party suppressing speech in the West because these companies make money from China. The CCP is going to punish them if they essentially publish this stuff. There is no other reason”
Chang thinks that China’s influence alone contributed to the spread of the virus.
“Communist Party is maligned and is grossly irresponsible. It has pressured governments to keep their borders open and it had to know that would result in the fast spread of coronavirus to other countries.”
In a stunning turn of events, Surgeon General Jerome Adams explained in an interview on live XM radio, that the Coronavirus Task Force has, effectively, dumped the Bill Gates/CDC/WHO predictive contagion model, and is now working with the real data.
He explained on the Sirius XM’s Breitbart News Daily host Alex Marlow, that given the new data, businesses will begin to re-open as early as May, others in June.
This runs contrary to the out-and-out fear-mongering of Dr. Fauci and Bill Gates who have made a media tour, threatening the public that businesses may not re-open for six months to a year, or until and unless governments purchase their conveniently patented, big-pharma vaccination.
According to Dr. Adams:
“What the American people need to know now is we actually have data, and so we’re tracking that data,”
Before this about-face, which appears to have come as an order from the Trump administration in consultation with the findings of Dr. Adams, the task force was working with’predictive models’, which had been created by the Bill Gates dominated WHO and CDC. Dr. Fausti’s control over the CDC has been criticized in the past for its for-profit motive in handling a range of illnesses from HIV to H1NI.
In those inflated, ‘fear-based’ models, the deaths of millions worldwide, and hundreds of thousands in America, were touted. These were used as the basis for what many experts have termed a ‘grossly disproportionate response‘.
Previously, the task force was working with predictive models, frequently criticized because of their tendency to exaggerate the possible effect of the virus on the United States. Models predicting the deaths of millions and hundreds of thousands in America appear to be overblown, as the real-time data is showing the death count much lower.
Adams said that the models usually took data from different cultures and places around the globe, but they were able to track more accurately what could happen in the United States based on real data gathered in places such as California and New York.
“We’re following this data every single day, and we’re giving that data to communities so that they can make informed and intelligent decisions about when and where to reopen,” he said.
A significant indicator for communities being allowed to reopen, Adams said, was actual testing data, not a predictive model.
“I feel confident that some places will start to reopen in May and June. Other places won’t; it will be piece by piece, bit by bit, but will be data-driven,” he said.
Adams praised South Korea and Singapore, which closed their borders early, just like the United States did with travelers from China. But he said there are lessons learned across the board.
Snowden fears that world leaders will hold onto new emergency powers well after the pandemic ends.
In addition to quarantines and lockdowns, some governments like those in China, Taiwan, and South Korea have been using a surveillance strategy called “contact tracing” to reduce the spread of the novel coronavirus.
While each country’s contact tracing program has slight variations, all of them are essentially cell phone apps that keep a running record of the user’s heath and the health records of all the people they come into contact with.
If a cell phone comes in close contact with someone who might have the virus, the user receives a text message informing them and then instructing them to self-quarantine for 14 days.
However, the quarantine is not necessarily voluntary, depending on where you live. In some countries, phones have been used as a sort of house arrest ankle-bracelet that will notify authorities if the person being monitored leaves the house for any reason.
These apps are being touted as the way to end the shut down in both Italy and the UK and it appears that officials are going to be taking things in that direction.
At face value, it may appear that this could be a useful strategy in preventing the spread of disease, but privacy advocates and tech experts are concerned that this information could be misused and that the unprecedented surveillance capabilities could be kept and held by corrupt governments long after the pandemic is over.
In a recent interview with Vice, NSA whistleblower Edward Snowden expressed his concerns about the coming surveillance program, calling it the “architecture of oppression.”
“Do you truly believe that when the first wave, this second wave, the 16th wave of the coronavirus is a long-forgotten memory, that these capabilities will not be kept? That these datasets will not be kept? No matter how it is being used, what’ is being built is the architecture of oppression,” Snowden said.
Snowden recognized that the virus was a serious threat and said that the intelligence community was well aware that it was only a matter of time before a massive pandemic crippled the country, even back when he was working in the NSA.
“There is nothing more foreseeable as a public health crisis in a world where we are just living on top of each other in crowded and polluted cities, than a pandemic. And every academic, every researcher who’s looked at this knew this was coming. And in fact, even intelligence agencies, I can tell you firsthand, because they used to read the reports had been planning for pandemics,” he said.
Snowden questioned the positive numbers that have come out of China in recent weeks and pointed out that the Chinese government has been credited with reducing the spread of the illness because they took such draconian measures during the lockdown.
Perhaps their extreme strategy is not working as well as they say it is, but since the government maintained tight control of any information coming out of the country, it is impossible to say for sure.
“If you’re looking at countries like China, where cases seem to have leveled off, how much can we trust that those numbers are actually true? I don’t think we can. Particularly, we see the Chinese government recently working to expel Western journalists at precisely this moment where we need credible independent warnings in this region,” Snowden said.
In a statement published on Friday, Apple and Google announced that they were teaming up in a rare partnership to develop compatible contact tracing apps, which they claim will work on an “opt-in” basis.
However, according toBloomberg, the companies are planning to eventually build the contact tracing into the device’s updates.
Apple and Google insist that you will still be able to opt-out of the program if you don’t want to participate, but it is possible that rankings on these apps could be used to gain entry into grocery stores or larger businesses and events once the economy opens up again.
“As authoritarianism spreads, as emergency laws proliferate, as we sacrifice our rights, we also sacrifice our capability to arrest the slide into a less liberal and less free world,” Snowden warned.
This is the sixty-four-thousand-dollar question. The premise that coronavirus is highly contagious and can cause disease provides the justification for putting entire nations on lockdown, destroying the global economy and throwing hundreds of thousands out of work. But is it contagious? Does it even cause disease?
As early as 1799, researchers puzzled over the cause of influenza, which appeared suddenly, often in diverse places at the same time, and could not be explained by any theory of contagion. In 1836, Heinrich Schweich, author of a book on influenza, noted that all physiological processes produce electricity and offered the theory that an electrical disturbance of the atmosphere may prevent the body from discharging it. He repeated the then-common belief that the accumulation of electricity in the body causes the symptoms of influenza and that outbreaks were due to atmospheric “influences”—hence the name influenza.
Now that we know about the electrical nature of the sun, we can make some interesting observations. The years 1645-1715 was a period that astronomers call the Maunder minimum, when the sun was very quiet; astronomers observed no sunspots during the time span and the northern lights were nonexistent; then in 1715, sunspots reappeared, as did the northern lights. Sunspot activity then increased, reaching a high in 1727, and in 1728, influenza appeared in waves on every continent. Sunspot activities became more violent until they peaked in1738 when physicians reported flu in both man and animals, including dogs, horses and birds, especially sparrows. By some estimates, two million people perished during the ten-year pandemic.
These and other facts about the relationship of influenza to disturbances in electricity come from a remarkable book, The Invisible Rainbow, by Arthur Firstenberg. Firstenberg chronicles the history of electricity in the U.S. and throughout the world, and the outbreaks of illness that accompanied each step towards greater electrification. The first stage involved the installation of telegraph lines—by 1875, these formed a spider web over the whole earth totaling seven hundred thousand miles, with enough copper wire to encircle the globe almost thirty times.
With it came a new disease called neurasthenia. Outside of the U.S., scientists recognized electricity as one of its causes. Like those suffering today from “chronic fatigue,” patients felt weak and exhausted, unable to concentrate. They had headaches, dizziness, tinnitus, floaters in the eyes, racing pulse, pains in the heart region and palpitations; they were depressed and had anxiety attacks. Dr. George Miller Beard noted that the disease spread along the routes of railroads and telegraph lines; it often resembled the common cold or influenza and commonly seized people in the prime of life.
1889 marks the beginning of the modern electrical era and also of a deadly flu pandemic, which followed the advent of electricity throughout the globe. Says Firstenberg, “Influenza struck explosively and unpredictably, over and over in waves until early 1894. It was as if something fundamental had changed in the atmosphere. . .”
Physicians puzzled over influenza’s capricious spread. For example, William Beveridge, author of a 1975 textbook on influenza, noted “The English warship Arachne was cruising off the coast of Cuba ‘without any contact with land. No less than 114 men out of a crew of 149 fell ill with influenza and only later was it learnt that there had been outbreaks in Cuba at the same time.”
During the first world war, governments on both sides of the conflict installed antennas which eventually blanketed the earth with strong radio signals–and during the later part of 1918, disaster struck. The Spanish flu afflicted a third of the world’s population and killed around fifty million people, more than the Black Death of the fourteenth century. Those living on military bases, where the antennas were routinely installed, were the most vulnerable. A common symptom was bleeding—from the nostrils, the gums, ears, skin, stomach, intestines, uterus, kidneys and brain. Many died of hemorrhage in the lungs, the victims literally drowning in their own blood. Tests revealed a decreased ability for the blood to coagulate.
Health officials in those days were very interested in the question of whether the Spanish flu was contagious. Doctors from the U.S. Public Health Service tried to infect one hundred healthy volunteers between the ages of eighteen and twenty- five by collecting mucous secretions from the noses, throats and upper respiratory tracts of those who were sick. They transferred these secretions to the noses, mouths and lungs of the volunteers, but not one of them got sick; blood of sick donors was injected into the blood of the volunteers, but they remained stubbornly healthy; finally they instructed those afflicted to breathe and cough over the volunteers, but none became sick. Researchers even tried to infect healthy horses with the mucous secretions of horses with the flu, but the results were the same. The Spanish flu was not contagious.
The year 1957 marked the installation of radar worldwide. The “Asian” influenza pandemic began in February 1957 and lasted for a year. A decade later the U.S. launched twenty-eight satellites into the Van Allen belts as part of the Initial Defense Communication Satellite Program (IDCSP), ushering in the “Hong Kong” flu pandemic, which began in July 1968.
As Firstenberg observes, “In each case—in 1889, 1918, 1957 and 1968—the electrical envelope of the earth. . . was suddenly and profoundly disturbed,” and along with it the electrical circuits in the human body. Western medicine pays scant attention to the electrical nature of living things—plants, animals and humans—but mountains of evidence indicate that faint currents govern everything that happens in the body to keep us alive and healthy. From the coagulation of the blood, to energy production in the mitochondria, even to small amounts of copper in the bones, which create currents for the maintenance of bone structure—all can be influenced by the presence of electricity in the atmosphere, especially “dirty” electricity, characterized by many overlapping frequencies and jagged changes in frequency and voltage. Today we know that each cell in the body has its own electrical grid, maintained by the highly structured water inside the cell membrane. Cancer occurs when this structure breaks down, and cancer has increased with each new development in the electrification of the earth.
Chinese medicine has long recognized the electrical nature of the human body and has developed a system to defuse the “accumulation of electricity” that leads to disease. It’s called acupuncture. Many things that we do instinctively also help release any unhealthy buildup of current—the mother who strokes her infant’s head or who scratches her children’s backs to put them to sleep, the caresses of lovers, walking barefoot, massage, even handshakes and hugs—all now discouraged by the frowny faces of health authorities as we face the specter of bed police bursting in at midnight to make sure that Dad is sleeping on the sofa.
Fast forward to the Internet and cell phone era. According to Firstenberg, the onset of cell phone service in 1996 resulted in greater levels of mortality in major cities like Los Angeles, New York, San Diego and Boston. Over the years wireless signals at multiple frequencies have filled the atmosphere to a greater and greater extent, along with mysterious outbreaks like SARS and MERS. Today we face the installation of fifth generation wireless (5G), broadcast in the gigahertz range, often at 60 gigahertz, a frequency that is highly absorbed by oxygen, causing the O2 molecule to split apart, making it useless for respiration
Compare the pattern of 5G installation in the top map to the pattern of corona virus cases in the lower map. While correlation does not prove causation, the strong overlap between 5G rollout locations and corona virus cases should give one pause, especially given the history of pandemics following step changes in planetary electrification.
On September 26, 2019, 5G wireless was turned on in Wuhan, China and also launched in parts of New York City (areas of uptown, midtown and downtown Manhattan, along with parts of Brooklyn, the Bronx and Queens), the difference being that the 5G grid in Wuhan was much denser, with about ten thousand antennas—more antennas than exist in the whole U.S.A., all concentrated in one city. Illness has followed 5G installation in South Korea, Italy and Iran. In South America, Ecuador is a hot spot for the respiratory illness, and it is in Ecuador that 5G first appeared. The 5G system is also installed on modern cruise ships and in many health care facilities. People who suffer from electrical sensitivity cannot go near many hospitals and nursing homes.
But surely this is just a coincidence. Isn’t it a virus that is causing the current outbreak? Doesn’t this nasty little creature called coronavirus infect us and make us sick? Please watch this talk by Dr. Andrew Kaufman in which he explains the role of exosomes in the cells.
Exosomes are particles released from the cell; they carry RNA, toxins and cellular debris in response to various insults (toxins, stress including fear, cancer, ionizing radiation, infection, injury, many diseases, immune response and asthma). A number of virologists agree with his conclusions that viruses are exosomes; they are the same size, the same shape, both carry RNA and both attach to the same receptors. These exosomes/viruses are the result and not the cause of illness, with primary roles of coagulation, intercellular signaling and excretion of waste materials. If 5G, by overloading the body’s electrical circuitry and by high-jacking oxygen, causes injury to the lung cells, then an increased production of exosomes (wrongly called viruses) is sure to be the result—and thank goodness!
No wonder the anti-viral medications—given in the early days of the pandemic, but now abandoned—caused such terrible side effects (allergic reactions, fever, nausea, vomiting, bleeding, diabetic lactic acidosis, damage to the kidney, liver and pancreas. . . and breathing problems). These drugs suppress the body’s efforts to protect itself against the poisonous effects of 5G and other toxins.
If you do a bit of surfing on the Internet, you will find that exosomes are the latest thing for diagnosis and therapy, with many medical uses—from cancer treatment, to wound healing, to hair restoration!
It’s clear that we are making the same mistake with viruses that we have made with cholesterol and saturated fat—blaming a substance that is essential to life for causing disease. Just twenty years ago the medical profession “knew” that bacteria were killers—now we recognize that bacteria are essential to health. How long will it take us to learn that so-called viruses are our friends?
It’s interesting to note that each wave of influenza has its own constellation of symptoms—during the Spanish flu epidemic the main problem was bleeding, the inability of the blood to coagulate; the main victims were healthy people in the prime of life, between the ages of twenty-five and forty. Today’s victims are older, usually with pre-existing conditions. The main symptom of today’s outbreak seems to be hypoxia, akin to high altitude sickness.
Please watch this video by Dr. Cameron Kyle-Sidell, working on the front lines in New York City. Says Kyle-Sidell, “We’ve never seen anything like it!” The afflicted are literally gasping for air. In fact, the ventilators that the hospitals have scrambled to obtain do more harm than good and may be accounting for the high mortality rate. These patients don’t need help breathing—they need more oxygen when they take a breath. This is not the sign of a contagious disease but of a disruption of our mechanisms for producing energy and getting oxygen to the red blood cells.
So is corona virus a contagious bad guy? Remember that researchers could not show that the dreadful Spanish flu was contagious. The fact that viruses are actually helpful exosomes, and that many who test positive are symptom-free, makes their role as a perpetrator highly unlikely. To settle this question once and for all, we need to do the same contagion studies that proved non-contagion in 1918. I’d be happy to be the first volunteer.
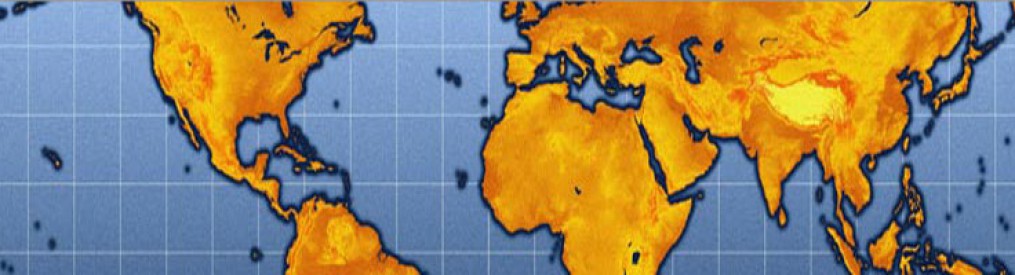

 We believe this crisis represents a world-changing opportunity to expose and transform antiquated ideologies that restrict health freedom. Germ theory is a scientifically bankrupt paradigm based in warfare models of pathogenic invasion. This theory has been leveraged as an instrument for geopolitical and social control – largely in the form of a vaccination agenda – to subdue the populace through coerced and forced bodily penetration and associated disability, mortality, and surveillance. As a result, conventional Western medicine functions as a sort of religion based on consensus assumptions and dogmatic medical monotheistic posturing. At its core, this approach is not salugenic or scientific and thus violates its stated ethical parameters around informed consent, beneficence, and an uncompromised evidence base.
We believe this crisis represents a world-changing opportunity to expose and transform antiquated ideologies that restrict health freedom. Germ theory is a scientifically bankrupt paradigm based in warfare models of pathogenic invasion. This theory has been leveraged as an instrument for geopolitical and social control – largely in the form of a vaccination agenda – to subdue the populace through coerced and forced bodily penetration and associated disability, mortality, and surveillance. As a result, conventional Western medicine functions as a sort of religion based on consensus assumptions and dogmatic medical monotheistic posturing. At its core, this approach is not salugenic or scientific and thus violates its stated ethical parameters around informed consent, beneficence, and an uncompromised evidence base. By Collin Rugg
By Collin Rugg
 By Denise Minger
By Denise Minger



































 By Brian Shilhavy
By Brian Shilhavy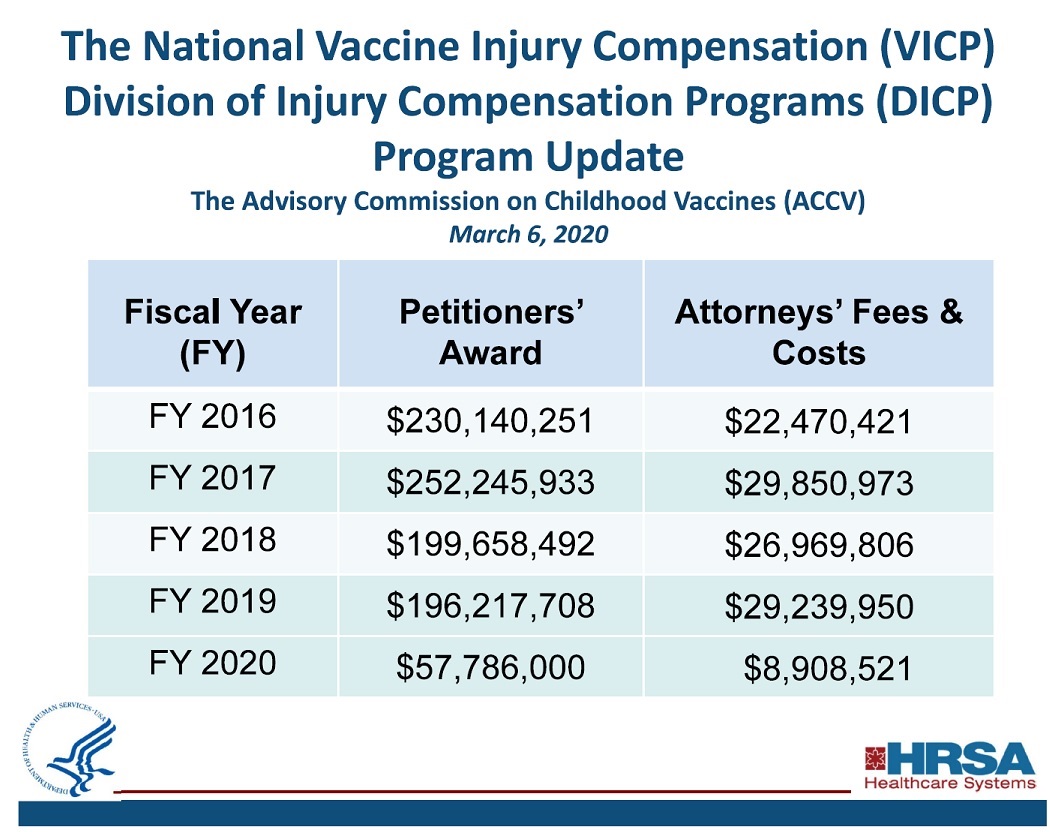
 By Andrew Joseph
By Andrew Joseph By John Vibes
By John Vibes



